
TL;DR:
- Incomplete intake checklists often lead to avoidable delays and compliance issues in post-acute care facilities.
- Designing checklists around legal requirements, structured workflows, and clear ownership reduces errors and improves admission efficiency.
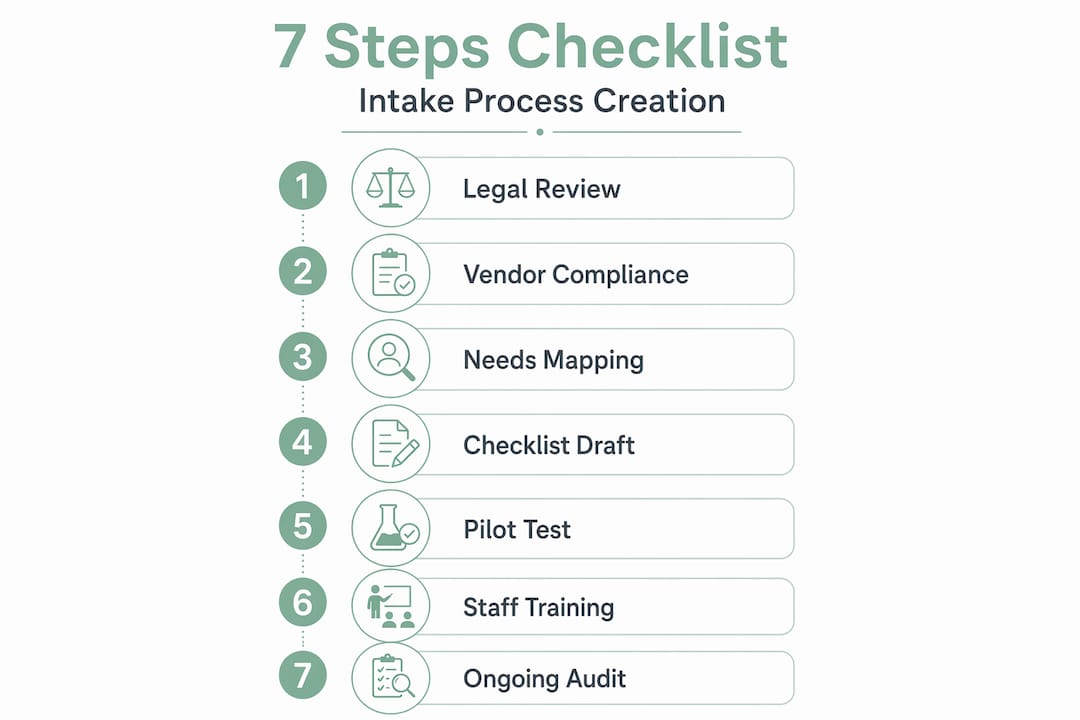
Incomplete intake checklists are one of the most avoidable causes of delayed admissions and compliance failures in skilled nursing facilities and post-acute care settings. Yet most admissions coordinators are handed a template from years ago and told to make it work. The intake checklist creation process, formally known as intake form procedure development, is too often treated as a one-time task rather than a structured workflow. This guide walks your team through every phase: from legal prerequisites and checklist design to workflow structuring, common pitfalls, and long-term quality control.
Table of Contents
- Key Takeaways
- The intake checklist creation process: prerequisites first
- Designing and structuring your intake checklist
- Common pitfalls that derail checklist implementation
- Verifying quality and maintaining your checklist over time
- My honest take on where intake checklists actually fail
- How Smartadmissions makes intake management faster and more reliable
- FAQ
Key Takeaways
| Point | Details |
|---|---|
| Compliance comes first | Collect only minimum necessary PHI and document all required HIPAA acknowledgments before designing other fields. |
| Structure drives completion | Organize the checklist into five core sections and use conditional logic to reduce irrelevant questions for each patient. |
| Treat intake as a workflow | Define submission, review, evaluation, and handoff stages with assigned owners to avoid bottlenecks. |
| Legal sign-offs get missed most | Separate each consent and acknowledgment into its own checklist item with a required signature field. |
| Lock dates protect data integrity | Use timed follow-ups within 7 business days and a final lock date to create a stable, auditable record. |
The intake checklist creation process: prerequisites first
Before your team writes a single field label, you need a clear picture of what you are legally required to collect and how you are permitted to collect it. Skipping this step produces checklists that either gather too much protected health information (PHI) or miss required disclosures entirely.
HIPAA requires collecting only the minimum necessary PHI for each specific purpose. That means your checklist should not default to capturing every piece of data your EHR system can hold. It should collect what is clinically and operationally required for that patient’s admission, nothing more.
Beyond PHI scope, there are non-negotiable legal acknowledgments your intake checklist must include. Each of these requires a separate, clearly labeled item with its own signature field:
- HIPAA Notice of Privacy Practices acknowledgment: Patients must receive and acknowledge this on or before the first visit.
- Consent to treat: A signed agreement that the patient authorizes the facility to provide care.
- Financial responsibility disclosure: Clear documentation that the patient or responsible party understands payment obligations.
- Medicare or Medicaid rights disclosure: Required for facilities participating in federal programs.
- Advance directive acknowledgment: Facilities must document whether a patient has an existing directive or declines to complete one.
For digital intake tools, the compliance checklist extends to your technology vendors. Audit trails, encryption, and role-based access are not optional features. Any vendor handling PHI must sign a Business Associate Agreement (BAA) before your facility uses their platform for intake data.
Pro Tip: Review your state’s specific consent requirements in addition to federal HIPAA standards. Several states mandate additional patient rights disclosures that federal law does not explicitly require.
| Requirement | Type | Who Signs |
|---|---|---|
| HIPAA Notice of Privacy Practices | Federal legal | Patient or legal representative |
| Consent to treat | Operational/legal | Patient or legal representative |
| Financial responsibility | Operational | Patient or guarantor |
| Advance directive acknowledgment | Federal regulatory | Staff with patient acknowledgment |
| Vendor BAA | Technical compliance | Facility and vendor |
Designing and structuring your intake checklist
Once prerequisites are documented, your team can move into the checklist design process itself. Structured design, not a long list of fields, is what separates a checklist that gets completed accurately from one that gets abandoned halfway through.

The five core sections every checklist needs
Every healthcare intake assessment checklist should be organized around these five sections:
- Patient demographics: Full legal name, date of birth, contact information, emergency contacts, and insurance carrier details.
- Insurance and financial information: Primary and secondary insurance, policy numbers, subscriber information, and authorization status.
- Medical history: Current diagnoses, surgical history, allergies, current medications with dosages, and relevant family history.
- Reason for visit or admission: Chief complaint or clinical reason for the referral, current functional status, and care goals.
- Consents and acknowledgments: All legal sign-offs listed as separate required items, not bundled into a single signature block.
This structure mirrors how your clinical and administrative staff will use the information downstream. Demographics flow to registration, insurance data goes to billing, medical history supports the clinical assessment, and consents protect the facility legally.
Using conditional logic to protect privacy and improve completion
Conditional logic in intake forms shows patients only the questions relevant to their situation. For example, a patient being admitted for post-surgical rehabilitation does not need to see behavioral health screening questions unless a trigger response makes them relevant. This approach reduces form length, improves completion rates, and prevents patients from being exposed to sensitive topics unnecessarily.
Pro Tip: When designing conditional logic, map out your decision tree on paper before building it in your digital tool. This prevents circular logic errors that can cause forms to malfunction mid-completion.
A structured intake workflow with defined stages turns a passive form into a managed process. Here is how the stages break down:
- Stage 1: Submission. Patient or referral source completes the intake checklist. Digital tools send automated confirmations and flag missing required fields.
- Stage 2: Review. Admissions coordinator reviews submitted data for completeness and accuracy within a defined timeframe, typically 24 to 48 hours.
- Stage 3: Clinical evaluation. The clinical team assesses the patient’s medical history and reason for admission to determine fit and level of care.
- Stage 4: Decision. The admissions team documents an accept, pending, or decline decision with supporting rationale.
- Stage 5: Handoff. Accepted patients are transitioned to onboarding with all documentation transferred to the appropriate care team.
For additional guidance on structuring this as an end-to-end process, the step-by-step intake workflow guide from Smartadmissions is a practical reference.
A well-structured checklist also means writing field labels in plain language. “Primary insurance carrier” is clearer than “Payor source.” “Current medications” is clearer than “Pharmacological regimen.” Your patients and their families are completing these forms, not clinicians.
Common pitfalls that derail checklist implementation
Even well-designed checklists fail in practice when the implementation process overlooks key operational details. These are the mistakes your team should actively prevent.
- Missed or incomplete legal acknowledgments. Inconsistent documentation of acknowledgments is the most common compliance failure in intake checklists. Each consent must be a discrete, required item, not embedded in a paragraph of text. If a patient skips it, the form should not submit.
- Untested mobile performance. A significant portion of patients complete digital intake forms on smartphones. A form that works on a desktop browser but breaks on a mobile device generates incomplete submissions and staff follow-up calls that consume hours every week.
- Unverified vendor compliance. Selecting a digital intake tool without confirming vendor HIPAA compliance and BAA status creates liability your facility may not discover until an audit. Verify before deploying, not after.
- No defined ownership of review stages. If the checklist workflow does not assign a specific role to each stage, submissions sit unreviewed. Define who is responsible for the review stage, who escalates incomplete forms, and who approves the final record.
- No intake lock date. Without a cutoff, admissions records stay open indefinitely and staff continue making undocumented changes. This destabilizes the data and creates audit problems.
Pro Tip: Run a pilot test with five to ten synthetic patient profiles before launching a new digital intake checklist. This surfaces mobile display issues, conditional logic errors, and submission failures before real patients encounter them.
The patient intake checklist for skilled nursing homes published by Smartadmissions provides a practical reference for facility-specific field requirements and compliance checkpoints.
Verifying quality and maintaining your checklist over time
A completed checklist submission is not the end of the process. Your team needs a defined follow-up cadence to address gaps, verify accuracy, and lock the record for compliance purposes.
Here is the three-step verification cadence that works for most post-acute care facilities:
- Kickoff intake review: Within 24 hours of submission, an admissions coordinator reviews the checklist against a required-fields list and contacts the patient or referral source to resolve any missing items.
- Follow-up gap session: Within 7 business days, schedule a dedicated session to collect any outstanding documentation, signatures, or clinical data. Document this session with a date-stamped addendum.
- Intake lock date: At day 14, the intake record is locked. Any subsequent changes require a formal amendment process with documented rationale and staff signature. This creates a stable version-controlled audit trail.
Role-based access controls are essential at this stage. Not every staff member should be able to edit a locked intake record. Define access tiers: read-only for most clinical staff, edit access for assigned admissions coordinators, and amendment authority for supervisors only.
Regular staff training reinforces these standards. When new admissions coordinators join your team, checklist completion and review procedures should be part of their formal orientation, not informal instruction from a colleague.
Pro Tip: Schedule a quarterly checklist audit where a supervisor reviews a random sample of 10 to 15 completed intake records against your required-fields standard. This surfaces recurring gaps before they become systemic compliance issues.
For a deeper look at documentation standards that align with these practices, the intake documentation guide from Smartadmissions covers version control, audit trail requirements, and staff accountability structures in detail.
My honest take on where intake checklists actually fail
I’ve reviewed a lot of intake processes across post-acute care settings, and the pattern is consistent. Facilities invest significant time in getting the clinical questions right and almost no time on the legal acknowledgment section. Then an audit reveals that 30% of records are missing a signed financial responsibility form or an advance directive acknowledgment. That’s a compliance exposure that clinical accuracy cannot fix.
The second problem I see regularly is the absence of workflow ownership. Creating an intake checklist is not the same as creating an intake process. A list of fields is passive. A workflow with named owners, defined timeframes, and escalation paths is what actually moves patients through admissions efficiently. Without that structure, the checklist becomes a document that staff complete out of obligation rather than a tool that drives decisions.
What actually works is starting from the legal requirements, building the checklist structure around them, and treating every stage from submission to lock date as a managed hand-off. Facilities that do this consistently see fewer compliance findings and faster average time to admission. The checklist is not the goal. A clean, auditable, complete patient record is the goal. The checklist is the method you use to get there.
— Harry
How Smartadmissions makes intake management faster and more reliable
Managing the intake checklist creation process manually across multiple referral sources is where administrative errors multiply. Smartadmissions was built specifically for skilled nursing facilities, rehabilitation centers, and post-acute care providers who need a better way to handle referral intake, documentation, and admissions workflow without adding staff hours.
The platform integrates directly with your existing EMR systems and insurance portals, automating eligibility verification and clinical documentation review so your team spends less time on data entry and more time on decisions. If you want to understand how different referral management approaches compare in practice, Smartadmissions offers detailed guidance on selecting the right system for your facility’s volume and case mix. You can also explore the difference between manual and automated admissions to see where the efficiency gains are largest for facilities like yours.
FAQ
What is an intake checklist in healthcare admissions?
An intake checklist is a structured form used during patient admissions to collect demographics, insurance details, medical history, and required legal acknowledgments. It standardizes the data collection process to support clinical decisions and compliance documentation.
What are the core sections of a healthcare intake checklist?
Most intake assessment checklists include five sections: patient demographics, insurance information, medical history, reason for admission, and consents or legal acknowledgments. Each section should be clearly labeled and logically grouped for patient and staff usability.
Why do legal acknowledgments get missed on intake checklists?
Required acknowledgments are most often missed when they are embedded in narrative text rather than listed as separate required fields. Each consent should be a discrete item with its own required signature to prevent it from being skipped.
How does conditional logic improve intake form completion rates?
Conditional logic displays only the questions relevant to each patient’s situation, reducing form length and preventing exposure to sensitive topics that do not apply. This improves completion rates and protects patient privacy.
What is an intake lock date and why does it matter?
An intake lock date is a defined cutoff, typically 14 days after initial submission, after which the intake record cannot be edited without a formal amendment. Timed lock dates create a stable, version-controlled audit trail that supports compliance verification and prevents undocumented changes to admissions records.