
TL;DR:
- Proper management of referral documentation is essential to reduce system failures that delay care and impact compliance. Creating complete, focused, and securely transmitted referrals with standardized workflows enhances accuracy and audit readiness. Regular follow-up, tracking rejection patterns, and leveraging automation tools like Smartadmissions streamline the process and improve patient outcomes.
Knowing how to handle referral documentation accurately is one of the most consequential skills your admissions team can develop. 1 in 3 referrals fall through the system entirely, and half of all physicians never receive confirmation that a patient completed a specialist visit. For skilled nursing facilities, rehabilitation centers, and post-acute care providers, that failure rate translates directly into delayed care, missed bed occupancy, and compliance exposure. This guide walks your team through the prerequisites, step-by-step process, common pitfalls, and quality verification methods that define high-performing referral documentation workflows in 2026.
Table of Contents
- Key Takeaways
- How to Handle Referral Documentation: Prerequisites First
- Step-by-step process for creating and managing referrals
- Troubleshooting common referral documentation mistakes
- Verifying documentation quality and audit readiness
- My perspective on referral documentation excellence
- How Smartadmissions helps you manage referral documentation
- FAQ
Key Takeaways
| Point | Details |
|---|---|
| Prepare before you document | Gather complete patient identifiers, clinical history, medications, and allergies before initiating any referral form. |
| Prioritize clinical clarity | A focused clinical question improves specialist triage more than a perfectly formatted template ever will. |
| Track every outbound referral | Link each referral to a follow-up date and initiate inquiry within 7 days if no specialist feedback arrives. |
| Standardize for audit readiness | Use consistent workflows and documentation templates across departments to withstand regulatory review. |
| Automate where possible | Referral management tools reduce manual errors, accelerate processing, and close care gaps through automated tracking. |
How to Handle Referral Documentation: Prerequisites First
Before your team completes a single referral form, the right information must be in hand. Incomplete submissions are one of the most preventable causes of referral rejection, and they cost your facility time that directly affects patient care timelines.
Every referral document should include the following core elements:
- Patient identifiers: Full legal name, date of birth, medical record number, and insurance details
- Presenting clinical question: The specific reason for referral, stated clearly and objectively
- Relevant medical history: Diagnoses, prior treatments, and surgical history pertinent to the referral
- Current medications and dosages: Including over-the-counter medications and supplements
- Known allergies and adverse reactions: Drug, food, and environmental
- Recent test results or imaging: Attach only what is directly relevant to the clinical question
Under the HIPAA Minimum Necessary standard, your team should send only the clinical information required for the specialist to complete their role. Sending an entire chart when a two-page summary suffices is not just inefficient. It creates compliance exposure.
The table below clarifies what belongs in a referral document versus what should stay in the primary record:
| Include in Referral | Keep in Primary Record |
|---|---|
| Active problem list relevant to referral | Full longitudinal problem list |
| Current medications | Medication history beyond 12 months |
| Allergies | Archived allergy history |
| Relevant imaging and lab results | Full imaging archive |
| Consent and authorization documentation | Billing and financial history |
Regarding forms and templates: your facility should have standardized referral templates, but the form itself is not the priority. Clinical quality of referral information matters more than the specific template used. A well-written referral on a plain document outperforms a poorly written one on an official form every time.
For secure transmission, use encrypted messaging portals, your EHR’s built-in referral module, or HIPAA-compliant fax solutions. Avoid standard email without encryption and never send referral documents through unverified communication channels.
Pro Tip: Create a pre-referral checklist inside your EHR that your team must complete before a referral form can be submitted. This single step can reduce incomplete submissions by a significant margin without adding time to the process.
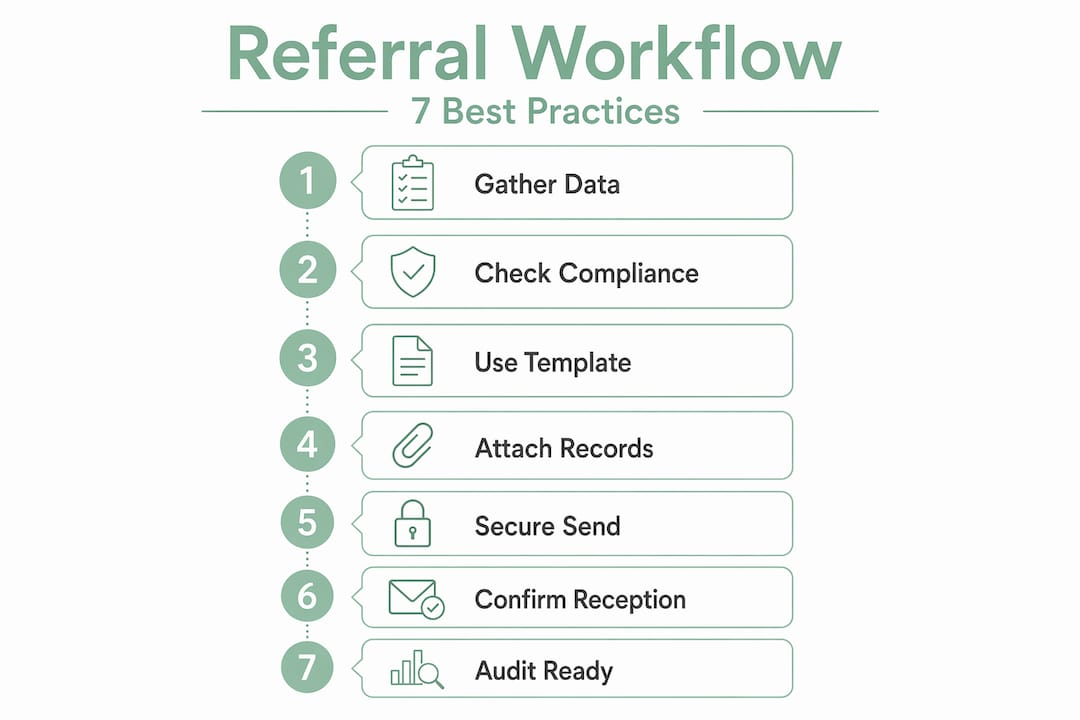
Step-by-step process for creating and managing referrals
Once your prerequisites are in place, managing referral paperwork becomes a repeatable, auditable process. Follow these steps consistently across your team:
Confirm the clinical indication. Before generating documentation, verify that the referral is clinically justified. A clear, specific clinical question reduces back-and-forth with the receiving provider and guides appropriate workup. For imaging referrals specifically, a clear clinical question guides the appropriate imaging technique and improves diagnostic accuracy.
Pull and review the patient record. Access the patient’s active problem list, medication reconciliation, and allergy documentation. Cross-reference against your pre-referral checklist to confirm all required fields are ready.
Complete the referral form with precision. Keep the referral letter concise. Referral letters of 1 to 2 pages that stay focused on the clinical question reduce cognitive load for triage staff and prevent delays in specialist review. Avoid padding the document with years of medical history the specialist will never use.
Attach supporting documentation selectively. Include only the test results, imaging reports, or clinical notes that directly support the reason for referral. Selective attachment is not just good practice. It reflects HIPAA compliance and respect for the receiving provider’s time.
Transmit through a secure, verifiable channel. Use your EHR’s referral module or a HIPAA-compliant portal. Confirm that the transmission was received by the receiving provider’s system. Document the transmission date, method, and recipient in the patient record.
Link the referral to the patient’s scheduling workflow. Attach a follow-up tickler or task to the referral entry in your system. If your facility uses referral tracking tools, this step can be automated, eliminating the need for manual follow-up.
Document consent and authorization. For referrals requiring prior authorization, attach the completed authorization form with the scope, patient identity, and expiration date clearly recorded. Documented consent whether via eConsent platform, signed paper form, or verbal consent with written documentation supports both compliance and patient transparency.
Pro Tip: Assign a single team member as the referral coordinator for each shift. That person owns transmission confirmation, authorization tracking, and follow-up scheduling for all referrals initiated during that period. Distributed responsibility is where referrals get lost.
Troubleshooting common referral documentation mistakes
Even well-prepared teams encounter referral rejections and processing delays. Recognizing the patterns behind these failures helps your team resolve them faster and prevent recurrence.
The most frequent causes of referral rejection or delay include:
- Missing or incomplete clinical information: The specialist cannot complete triage without the clinical question, relevant history, or supporting documents
- Incorrect patient identifiers: A mismatched date of birth or insurance ID triggers administrative rejection before a clinician ever reviews the referral
- Authorization gaps: Submitting without required prior authorization, or with expired authorization, delays care and creates billing risk
- Wrong referral pathway: Sending a referral to the wrong specialty or subspecialty wastes days in transit and may result in a redirect that confuses the patient
When a referral is rejected or redirected, treat it as a process signal rather than an obstacle. Rejected referrals often serve as clinical governance tools that reveal gaps in care pathway design. Document the reason for rejection, update your team’s process notes, and use patterns of rejection to refine your referral templates over time.
Tracking referral completion is where many facilities have the most room for improvement. Downstream reconciliation and automated follow-up systems that flag missing specialist feedback prevent referrals from simply disappearing once transmitted.
“If no feedback from the specialist arrives within 7 days, initiate a direct inquiry. Routine reconciliation of open referrals is the most reliable method for preventing care gaps and lost referrals.” — Referral Handling Best Practices
Coordination with specialists and internal care teams is also worth formalizing. Set a standard for how your team communicates updates on open referrals, who owns the specialist relationship, and what triggers an escalation. Clear internal ownership reduces referral review time and keeps care timelines on track.
Verifying documentation quality and audit readiness

Handling referral documentation well is not only about accuracy at the point of creation. It is about maintaining records that hold up under regulatory scrutiny and support billing integrity over time.
The table below compares documentation practices by compliance risk level:
| Practice | Lower Risk | Higher Risk |
|---|---|---|
| Template use | Standardized, validated templates | Ad hoc or inconsistent formats |
| Transmission records | Logged with date, method, recipient | Untracked or verbal only |
| Authorization documentation | Signed and filed with expiration date | Missing or expired |
| Consent records | Documented per policy (eConsent or written) | Verbal with no written record |
| Audit trail | Complete EHR audit log with user timestamps | Gaps or manual overrides |
Standardized workflows and cross-departmental governance reduce the variability that undermines compliance during audits. When every department follows the same documentation process, your facility’s records become both more accurate and more defensible.
Your referral data must also align with billing requirements. Referral relationships involving financial considerations fall under Anti-Kickback Statute and Stark Law scrutiny. Proactive downstream tracking that links referral activity to outcomes and billing records is not optional in 2026. It is a compliance requirement with real enforcement consequences.
Finally, ongoing staff training matters. Documentation standards evolve, and the team members who handle referrals daily need regular updates on form requirements, authorization rules, and secure transmission protocols. Build quarterly documentation audits into your governance calendar to catch drift before it becomes a pattern.
My perspective on referral documentation excellence
I’ve worked with referral workflows long enough to know that most documentation problems are not caused by carelessness. They are caused by systems that make it too easy to skip steps and too hard to verify completion. The teams that handle referral documentation best are not necessarily the ones with the most rigorous checklists. They are the ones that have built accountability into the process itself.
What I’ve consistently seen is that facilities place too much emphasis on form formatting and not enough on the clinical question at the center of each referral. Specialists are triaging dozens of referrals a day. The ones that get moved to the top of the queue are the ones where the clinical question is clear, the supporting documents are targeted, and the sending provider has clearly communicated why this patient needs their expertise now.
The best practices for referral documents are not just about compliance. They are about communicating effectively with the provider on the other end. When a referral is written as a clinical communication rather than a form-filling exercise, the patient benefits. The specialist benefits. And your facility avoids the administrative cycle of rejections, resubmissions, and follow-up calls that consume your team’s time.
Redirection and rejection are also underused feedback mechanisms. In my experience, most teams log a rejection and resubmit without ever analyzing why it happened. That is a missed opportunity. Patterns of rejection reveal exactly where your intake process needs refinement, and organizing your referral tracking data by rejection reason is one of the most efficient ways to improve documentation quality at scale.
— Harry
How Smartadmissions helps you manage referral documentation
Managing referral paperwork manually across a skilled nursing facility or post-acute care setting places real strain on your admissions team. Missed steps, incomplete records, and delayed follow-ups add up quickly when your team is handling high referral volumes without the right tools.
Smartadmissions is built specifically for facilities like yours. The platform automates the documentation steps that consume the most time, including intake form population, authorization tracking, and specialist follow-up alerts. Its AI-powered assistant integrates directly with your existing EMR and insurance portals, so your team is not re-entering data or chasing confirmations manually. If you are evaluating options, the top referral management tools for 2026 offer a strong starting point for comparison. You can also explore referral management system examples that match the size and workflow of your facility.
FAQ
What are the core elements of a referral document?
A referral document should include patient identifiers, the clinical question, relevant medical history, current medications, allergies, and any supporting test results directly tied to the reason for referral.
How do you stay HIPAA compliant when sending referrals?
Follow the HIPAA Minimum Necessary standard by sending only the clinical information the specialist needs to complete their role. Use encrypted portals or your EHR’s secure referral module for all transmissions.
What steps to handle referral forms most efficiently?
Complete a pre-referral checklist before submission, write a focused 1 to 2 page referral letter, attach only relevant documents, transmit through a verified channel, and link the referral to a follow-up task with a 7-day response window.
Why do referrals get rejected and how can you prevent it?
The most common causes are missing clinical information, incorrect patient identifiers, and expired or missing authorization. Standardized templates and pre-submission checklists address the majority of these errors before the referral leaves your facility.
How do you process referral requests that are redirected by a specialist?
Document the reason for redirection, update your referral to the correct specialty or subspecialty, and treat the feedback as a process improvement signal. Tracking redirection patterns helps your team refine referral pathways over time.