
TL;DR:
- Manual insurance verification delays patient placement and stalls revenue for skilled nursing facilities. True integration connects intake systems, EHRs, and payer APIs, enabling automated eligibility checks and prior authorizations, thereby improving speed and accuracy. Ongoing workflow redesign and monitoring are essential to maximize operational efficiency and comply with CMS interoperability standards by 2027.
Manual insurance verification in skilled nursing and rehabilitation settings is not just slow — it actively blocks patient placement. When your admissions team spends hours on the phone confirming eligibility or faxing prior authorization requests, beds sit empty and revenue stalls. Yet most facilities have invested in insurance portals without realizing those portals are doing far less than they could. Understanding the full role of insurance portal integration — not just what a portal displays, but how it connects to your intake systems, your EHR, and your billing workflows — is where the real operational gains begin. This guide gives you a clear, actionable picture.
Table of Contents
- Why insurance portals alone aren’t enough: The true role of insurance portal integration
- Understanding CMS-0057-F and its impact on insurance portal integration
- Technical essentials: How real-time eligibility and authorization workflows work
- Common pitfalls and pro tips to maximize your insurance portal integration
- How effective insurance portal integration transforms skilled nursing admissions
- Fresh perspective: Why treating insurance portals as workflows, not windows, unlocks true value
- Streamline your patient intake with smarter referral and admissions automation
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Integration vs portal only | True insurance portal integration connects portals to backend APIs, not just manual screens. |
| CMS-0057-F deadlines | Payers must implement FHIR-based APIs by 2027 to enable electronic prior authorization workflows. |
| Real-time verification | Eligibility verification uses real-time 270/271 transactions for near-instant data access. |
| Security requirements | HIPAA compliance requires encryption, access controls, and audit logging for API usage. |
| Operational impact | Integrated portals accelerate patient intake, reduce denials, and improve care coordination. |
Why insurance portals alone aren’t enough: The true role of insurance portal integration
Insurance portals were originally built as browser-based access points. A staff member logs in, types in a patient’s information, and reads the eligibility result on screen. That is not integration. That is a manual lookup with a digital interface.
For post-acute intake, insurance portal integration means wiring intake and billing workflows to payer-provided APIs so eligibility and authorization decisions are checked electronically rather than manually. The portal becomes part of an automated chain, not a standalone stop.
Here is what that distinction means in practice for your facility:
- No integration: A staff member manually logs into a payer portal, reads eligibility, transcribes the result into your EHR, and then initiates a separate prior authorization request, usually by fax.
- True integration: Your intake system sends a structured eligibility query automatically when a referral arrives. The payer responds electronically. The result populates your EHR directly, and a prior authorization request is triggered without manual entry.
The gap between these two scenarios is not just convenience. It is speed, accuracy, and the ability to make confident placement decisions without waiting for a callback. Facilities that have moved beyond portal-only methods report fewer entry errors, faster turnaround, and staff freed from repetitive data lookups to focus on clinical and financial review. You can explore intake workflow improvement ideas specific to post-acute settings to see where automation creates the most immediate impact.
Understanding CMS-0057-F and its impact on insurance portal integration
If you have not yet mapped your integration readiness to the CMS-0057-F final rule, now is the time. This regulation is the most significant driver of change in insurance software integration for skilled nursing facilities in recent years.
Here are the four FHIR-based APIs (Fast Healthcare Interoperability Resources) that the rule mandates payers must support:
- Patient Access API — Gives patients electronic access to their own claims, clinical data, and prior authorization information.
- Provider Access API — Allows providers, including your admissions team, to query payer systems for patient data with appropriate consent.
- Payer-to-Payer API — Enables continuity of care data exchange when a patient transitions between payers.
- Prior Authorization API — Allows providers to submit prior auth requests electronically and receive time-stamped decisions back into their systems.
By January 1, 2027, impacted payers must implement all required FHIR-based interoperability APIs, including Prior Authorization. That deadline is closer than it looks given the backend system work required.
The rule also enforces strict turnaround timeframes: 72 hours for expedited prior authorization requests and 7 calendar days for standard requests. These are legally binding, which means your facility needs to be ready to both submit requests electronically and act on decisions quickly when they arrive.
This is not just a front-end upgrade. Your EHR and intake platform must be capable of generating structured authorization data in FHIR format, submitting it to payer endpoints, and consuming the response in a way your team can act on. Facilities investing now in healthcare intake technology are building the backend readiness that CMS-0057-F demands.
Technical essentials: How real-time eligibility and authorization workflows work
Understanding the mechanics helps you ask the right questions when evaluating or upgrading your integration setup.
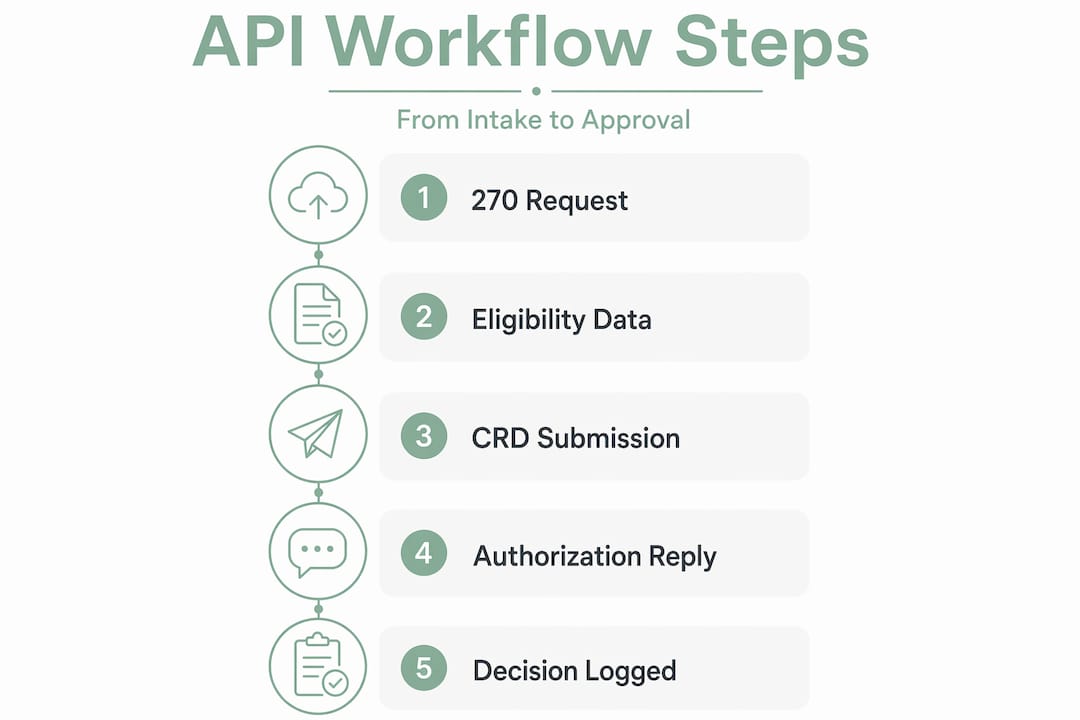
Eligibility verification uses a standardized transaction pair. Your system sends a 270 request containing patient and payer identifiers. The payer responds with a 271 message that includes beneficiary demographics, coverage status, and benefit details. Medicare eligibility via HETS (Health Eligibility Transaction System) uses this 270/271 format to deliver near-instant results, removing the need for manual portal lookups entirely.
Prior authorization now uses FHIR APIs instead of fax or portal form submissions. Your system submits a structured CRD (Coverage Requirements Discovery) or PAS (Prior Authorization Support) request. The payer processes it and returns an authorization number or denial with reason codes, all electronically and within the CMS-mandated timeframes.
| Workflow | Transaction type | Data format | Typical response time |
|---|---|---|---|
| Eligibility verification | 270/271 | X12 EDI | Seconds to minutes |
| Prior authorization | FHIR PAS API | FHIR R4 JSON | 72 hours (expedited) / 7 days (standard) |
| Payer data access | Provider Access API | FHIR R4 JSON | Real-time query |
Security is non-negotiable across all of these workflows. HIPAA-compliant API integrations require encryption in transit and at rest, access controls with scoped permissions per user role, and full audit logs of every data access event. Your integration must also include identity management to ensure that only authorized staff and systems are querying payer endpoints.
Pro Tip: When evaluating any real-time eligibility verification tool, confirm it supports both X12 270/271 for Medicare and FHIR-based API access for Medicaid managed care plans. Many facilities are surprised to find their tools only cover one or the other.
Common pitfalls and pro tips to maximize your insurance portal integration
Most integration failures are not technical. They are operational. The payer API is there, the connection is built, and the project is declared done. Then denials continue at the same rate because nobody redesigned the workflow around the new data.
Inconsistent eligibility and authorization data across member portals and billing systems is the biggest hidden failure in portal integration projects. If your intake system shows one eligibility status and your billing platform shows another, the downstream result is a denial that could have been avoided.
Here are the most common pitfalls and how to address them:
- Treating authorization as a single event: Prior authorization is a lifecycle. A request is submitted, reviewed, approved, appealed, or denied with reason codes. Your workflow must track status changes, not just the initial response.
- Neglecting denial reason transparency: Structured request and response handling for prior authorization must include documentation of denial reasons so your team can respond with the right clinical information quickly.
- Skipping workflow redesign: Building the integration without changing how staff act on the data means you get faster wrong answers. Redesign your intake steps to reflect the new data flow before go-live.
- Underestimating identity management: Every API call must be tied to an authenticated user or system credential. Budget for this from day one, not as an afterthought.
- No monitoring in place: Integration errors happen silently. A dropped API call or a misconfigured endpoint means your team thinks eligibility was confirmed when it was not.
Pro Tip: Set up automated monitoring for API error rates and response times from day one. When an integration goes silent or starts returning unexpected error codes, you want an alert in your inbox, not a denial notice from a payer.
Pro Tip: Train your front-line admissions staff to read and interpret authorization status messages, not just approval or denial. Understanding reason codes allows your team to prioritize clinical documentation quickly and avoid placement delays. You can find more detail on how intake automation benefits your team’s day-to-day decision-making.
How effective insurance portal integration transforms skilled nursing admissions
The operational impact of moving from manual portal access to true API-driven integration is measurable and significant. Here is what your facility can realistically expect.
| Metric | Manual portal workflow | Integrated API workflow |
|---|---|---|
| Eligibility check turnaround | 15–45 minutes | Under 2 minutes |
| Prior auth submission time | 30–90 minutes per case | 5–10 minutes per case |
| Authorization denial rate | High due to incomplete data | Reduced with structured submissions |
| Staff time per intake | 2–4 hours | 30–60 minutes |
| Discharge planning lead time | Delayed pending auth | Earlier with real-time auth status |
Facilities that integrate interoperability APIs can anticipate reduced intake cycle times and earlier discharge planning linked to timely prior authorization decisions. That means faster bed turnover, which directly affects your revenue cycle.
The financial case is also backed at the federal level. CMS projects $15 billion in savings over ten years from interoperable prior authorization workflows reducing administrative burden across the healthcare system. The savings to individual facilities come through lower denial rates, reduced rework, and fewer staff hours consumed by manual verification.
Key benefits your admissions team and administrators gain from effective integration:
- Operational efficiency: Faster eligibility and authorization decisions reduce intake bottlenecks and increase bed fill rates.
- Regulatory compliance: Meeting CMS-0057-F requirements by 2027 positions your facility ahead of competitors still relying on manual workflows.
- Patient satisfaction: Faster admission decisions reduce uncertainty for patients and families during transitions of care.
- Financial performance: Fewer denials, lower administrative overhead, and improved documentation accuracy all strengthen your revenue cycle.
Explore how healthcare workflow automation applies specifically to post-acute admissions to see the full picture of operational gains.
Fresh perspective: Why treating insurance portals as workflows, not windows, unlocks true value
Most facilities approach portal integration as an IT project. Get the connection built, confirm the data flows, and move on. That framing is why so many integrations underperform.
The portal is not the system. It is a surface. The real value lies in what happens behind it: the API layer that can automate decisions, populate your intake records, and trigger next steps without anyone picking up a phone. The portal should function as a workflow surface, not the system of record, because the API layer enables standardized, automatable decision flows that a browser screen never can.
Here is the uncomfortable truth we see in post-acute settings: many facilities have completed integration projects and still rely heavily on manual follow-up because their staff was never trained to act differently. The technology changed, but the behavior did not. A new intake workflow built around intake workflow automation requires equal investment in people and process as it does in software.
The facilities that get the most from insurance portal integration are the ones that measure it continuously. They track API response rates, monitor denial patterns tied to specific authorization pathways, and hold regular reviews of how intake decisions align with real-time payer data. They treat integration as an ongoing operational discipline, not a one-time implementation.
If you are a forward-thinking administrator, here is how to shift your framing: stop asking whether your portal is connected, and start asking whether your intake decisions are driven by real-time payer data. That question gets to the heart of what integration is actually for.
Streamline your patient intake with smarter referral and admissions automation
Understanding the role of insurance portal integration is the first step. Putting it into practice requires the right tools. Smart Admissions is built specifically for skilled nursing homes, rehabilitation centers, and post-acute care providers who need real-time eligibility verification, electronic prior authorization support, and AI-powered referral management in a single platform.

Our platform integrates directly with EHR systems and payer APIs so your team gets eligibility results and authorization status inside their existing workflow — not in a separate portal window. Facilities using Smart Admissions have reported up to 20% faster bed occupancy through reduced intake bottlenecks. You can review examples of referral management systems to see how API-driven intake compares to traditional methods, or follow our step-by-step admissions workflow guide to map your current process against best practices. Your team deserves tools that match the pace CMS now requires.
Frequently asked questions
What is the main benefit of integrating insurance portals in healthcare intake?
It enables real-time eligibility and authorization checks through electronic data exchange, eliminating the manual fax and portal-only steps that delay patient admissions and increase error rates.
When must healthcare payers implement the CMS-mandated interoperability APIs?
FHIR-based APIs including Prior Authorization must be implemented by January 1, 2027, meaning your facility’s intake systems need to be ready to consume and act on structured payer data before that deadline.
How does real-time Medicare eligibility verification work in insurance portal integration?
Your system sends a 270 request to HETS and receives a 271 response containing live Medicare eligibility data including coverage details and beneficiary demographics, typically within seconds.
What security measures are necessary for HIPAA-compliant insurance portal integrations?
All API integrations must include encryption in transit and at rest, role-based access controls with scoped permissions, and complete audit logs that track every data access event across your systems.
What common pitfalls should healthcare administrators avoid in integrating insurance portals?
The most damaging errors are inconsistent eligibility data across intake and billing systems and failing to redesign workflows to act on authorization status updates, both of which produce preventable denials and operational delays.