
TL;DR:
- Interoperability enables automatic data exchange, reducing manual intake time and errors.
- Implementing real-time health data exchange can boost efficiency by up to 15% and cut costs significantly.
- Success depends on staff engagement and workflow integration, not just technology adoption.
Skilled nursing facilities and rehabilitation centers face a relentless pressure: admit patients faster, reduce errors, and keep beds filled, all while managing mountains of paperwork and fragmented data systems. Manual intake processes cost your team hours every day, and a single missing document can delay a patient’s transition by 24 hours or more. Real-time interoperability improves efficiency by 15% and contributes to multi-million dollar savings for post-acute care systems. In this article, you will learn what interoperability actually means for your admissions team, how it transforms intake workflows, what the evidence says about clinical outcomes, and which best practices deliver the strongest return on investment.
Table of Contents
- Understanding interoperability in healthcare admissions
- How interoperability streamlines admissions and intake
- Measuring impact: Efficiency gains and clinical outcomes
- Best practices: Maximizing interoperability ROI in admissions
- The uncomfortable truth: What most admissions teams miss on interoperability
- Ready to streamline your admissions? Explore automated solutions
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Streamlined intake | Interoperability enables faster, automated admissions by sharing data across systems. |
| Efficiency gains | SNFs and rehab centers can achieve up to 15% improvement and substantial cost savings with real-time data exchange. |
| Mixed clinical results | Some studies show reduced readmissions, but impact varies depending on implementation and workflow alignment. |
| ROI strategies | Admissions teams see the best results by targeting high-impact workflows such as ADT notifications and medication reconciliation. |
| Action over compliance | True benefits require staff engagement and practical workflow changes, not just regulatory compliance. |
Understanding interoperability in healthcare admissions
Interoperability in healthcare refers to the ability of different information systems, devices, and software applications to connect, communicate, and exchange data accurately and in a usable format. For admissions coordinators at skilled nursing facilities and rehab centers, this means patient records, medication lists, insurance information, and clinical assessments can flow automatically from a referring hospital into your intake system, without manual re-entry.
The types of data exchanged in an interoperable admissions workflow include:
- ADT (Admit, Discharge, Transfer) notifications: Real-time alerts that tell your team when a patient is being discharged from a hospital and is ready for placement.
- Medication reconciliation data: A complete, current list of the patient’s medications, reducing dangerous gaps or duplications during transitions.
- Clinical assessments and care plans: Functional status scores, therapy needs, and physician orders that inform your admissions decision immediately.
- Insurance and eligibility information: Payer data that supports faster authorization and reduces billing delays.
The core technologies enabling this exchange include HL7 FHIR (Fast Healthcare Interoperability Resources) standards and the PACIO Project, which specifically defines FHIR implementation guides for transitions of care tailored to SNF and rehab admissions roles. These standards ensure that data is structured consistently, so your EHR system can read and act on information from a hospital’s system without manual translation.
“Interoperability is not just a technology upgrade. It is a workflow transformation that directly reduces the time your admissions coordinators spend chasing faxes and re-entering data.”
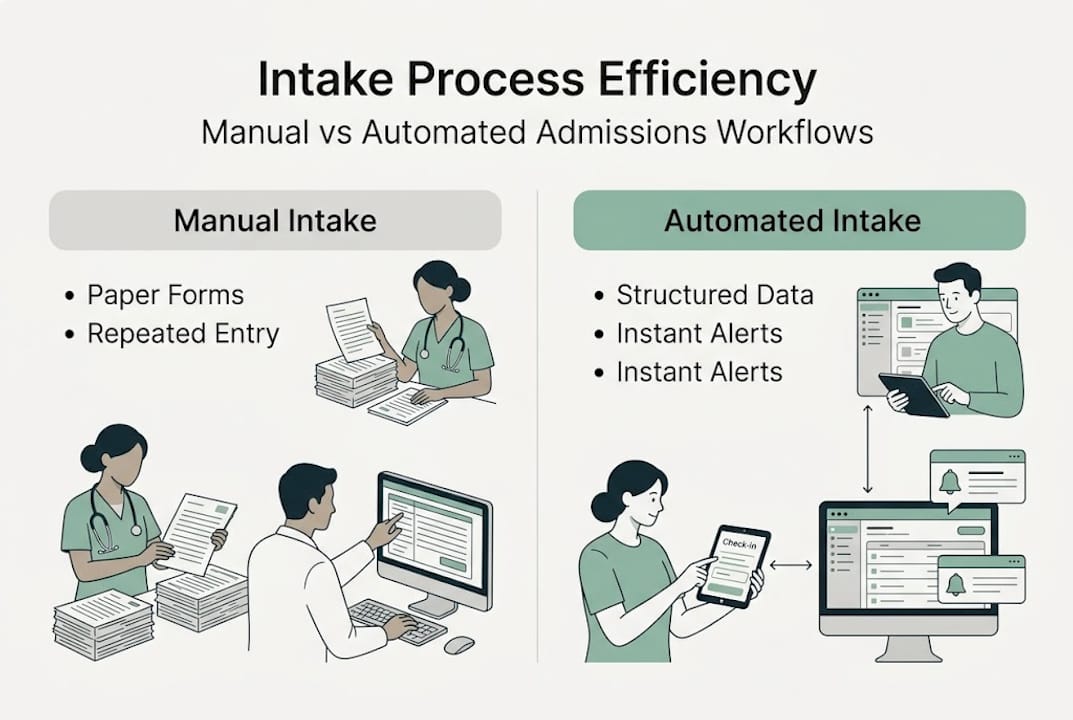
Compare the two realities your team may know well. In a manual intake process, a coordinator receives a fax referral, calls the hospital for missing documents, re-enters data into your EHR, waits for insurance verification, and repeats steps as errors surface. With automation in healthcare admissions, the referral arrives digitally, data populates your system automatically, and eligibility is verified in real time. The difference is not incremental. It is structural. Facilities that invest in workflow automation for admissions report faster decision-making and fewer bottlenecks at every stage of the intake process.
How interoperability streamlines admissions and intake
With a clear understanding of interoperability, let’s see how it actually transforms admissions workflows from start to finish.
Here is a step-by-step view of how an interoperable admissions workflow operates in practice:
- Referral received digitally: The hospital’s EHR sends a structured referral directly to your admissions platform via FHIR API, including clinical notes, diagnoses, and therapy orders.
- Patient data auto-populates: Your system reads the incoming data and fills intake forms automatically, eliminating duplicate entry and reducing transcription errors.
- Insurance eligibility verified in real time: Integrated payer connections confirm coverage and authorization requirements within minutes, not hours.
- Clinical review triggered: Your admissions coordinator reviews a pre-populated clinical summary and makes an accept or decline decision with complete information in hand.
- Bed assignment and care team notification: Once accepted, the system alerts the nursing team, therapy department, and dietary staff simultaneously.
- Transition documentation stored: All records are archived in a HIPAA-compliant format, ready for billing and quality reporting.
The contrast with paper-based or fax-driven intake is significant. Interoperability reduces manual reconciliation and improves data flow during hospital-to-SNF transitions, which directly lowers the risk of medication errors and care gaps that harm patients and generate liability.
Pro Tip: Set up automated ADT notification alerts so your admissions team receives discharge signals from partner hospitals before the case manager even calls. This gives your coordinators a head start on clinical review and bed planning.
| Factor | Manual intake | Interoperable intake |
|---|---|---|
| Data entry | Repeated, error-prone | Automated, structured |
| Insurance verification | 1 to 4 hours | Minutes |
| Referral-to-decision time | 24 to 48 hours | Under 4 hours |
| Medication reconciliation | Manual, fragmented | Automated, complete |
| Documentation compliance | Inconsistent | Standardized |
Facilities that automate admissions for faster bed occupancy consistently report higher bed fill rates and lower administrative overtime. The workflow automation benefits extend beyond speed, improving patient safety and staff satisfaction at the same time.
Measuring impact: Efficiency gains and clinical outcomes
To quantify these improvements, let’s examine real-world results and the nuances behind interoperability in admissions.
The financial and operational evidence is compelling. Systems that implement real-time health data exchange report efficiency improvements of up to 15% and reductions in readmissions, inpatient stays, and emergency department visits, sometimes reaching 21 to 29% reductions in those categories. TriHealth, a large post-acute care network, projected $8 million in annual savings after implementing a collaborative data exchange system.
Here is a summary of key benchmarks observed in SNF and rehab settings:
| Metric | Reported improvement |
|---|---|
| Intake efficiency | Up to 15% gain |
| Hospital readmissions | 21 to 29% reduction |
| Emergency department visits | Measurable decrease |
| Annual cost savings (large network) | Up to $8 million |
| Medication error rates | Reduced with automated reconciliation |
Clinical outcomes also improve when admissions teams receive complete, accurate data at the point of intake. When your coordinators know a patient’s full medication list, functional status, and care plan before arrival, the nursing team can prepare appropriately, reducing adverse events in the first 72 hours of admission.
However, the evidence is not uniformly positive. Some research shows no significant effect on SNF readmissions from health information exchange participation, and certain value-based programs failed to produce the expected reductions. These findings matter. They suggest that technology access alone does not guarantee results. Implementation quality, staff training, and workflow alignment are critical variables.
- Facilities with strong clinical leadership involvement see better outcomes than those treating interoperability as an IT project.
- Interoperability tools work best when integrated into existing EHR systems rather than layered on top as separate portals.
- Preserving complete medical history and patient safety data during transitions is a key driver of outcome improvements.
For top-performing SNFs in admissions, the common thread is not just having interoperability tools but using them consistently and purposefully across every admission.
Best practices: Maximizing interoperability ROI in admissions
Now, let’s turn these insights into action with practical best practices for admissions teams.
Not all interoperability use cases deliver equal value. ROI is maximized by targeting high-impact workflows such as ADT notifications and medication reconciliation, which have demonstrated multi-million dollar savings in post-acute care settings. Your team should prioritize these before expanding to other data exchange functions.
Here are the highest-impact actions your admissions team can take:
- Activate ADT notifications first: This single workflow change gives your team real-time visibility into discharge events at partner hospitals, enabling proactive outreach and faster bed placement.
- Automate medication reconciliation: Connect your intake system to hospital pharmacy data so medication lists arrive pre-populated and flagged for conflicts.
- Standardize clinical review checklists: Use interoperable data to build consistent intake criteria that reduce variability in accept or decline decisions.
- Track referral-to-admission time as a KPI: Measure this weekly and use it to identify workflow bottlenecks that interoperability tools can address.
- Align with value-based care benchmarks: Use readmission rates and length-of-stay data from your interoperable system to demonstrate performance to payers and referral partners.
Pro Tip: Before expanding your interoperability footprint, audit which hospital partners send the highest referral volume. Prioritize deep integration with those partners first. You will see faster ROI and fewer implementation headaches.
Common pitfalls to avoid include treating interoperability as a one-time IT project, skipping staff training on new data workflows, and failing to update intake protocols to reflect the new data available. Automation for admissions efficiency requires ongoing attention, not a set-and-forget approach. The automated workflow benefits compound over time when your team actively uses the data flowing into your system to make faster, better-informed decisions.
The uncomfortable truth: What most admissions teams miss on interoperability
Here is the perspective that shifts how admissions teams approach interoperability altogether.
Most facilities invest in interoperability to satisfy regulatory requirements or to check a compliance box. They implement FHIR-compliant connections, complete the onboarding, and then wonder why their readmission rates or bed fill times have not meaningfully improved. The technology is working. The workflow is not.
The research confirms this pattern. Some value-based programs, including SNF VBP, failed to reduce readmissions despite widespread HIE participation, which tells us that access to data does not automatically translate into better decisions. The gap is almost always human and organizational, not technical.
The admissions coordinators who get the most from interoperability treat incoming data as a decision-support tool, not a documentation formality. They review ADT alerts within minutes, not hours. They flag medication conflicts before the patient arrives. They use clinical summaries to prepare the care team proactively.
True gains come from staff buy-in and targeted use, not from regulatory compliance alone. If your team sees interoperability as more data to manage rather than faster answers to act on, the investment will underperform. Facilities that follow successful SNF admissions strategies build a culture where real-time data is expected, trusted, and acted upon at every step of intake.
Ready to streamline your admissions? Explore automated solutions
With perspective in mind, here is how you can take the next step and put interoperability to work for your facility.
Smart Admissions is built specifically for skilled nursing facilities and rehab centers that want to move beyond manual intake and realize the efficiency gains that interoperability promises. The platform connects with your existing EHR and insurance portals to automate referral review, eligibility verification, and documentation management in one place.

If your team is ready to automate admissions for faster bed occupancy, Smart Admissions gives you the tools to act on real-time data without adding administrative burden. Explore our intake automation guide to see how facilities like yours have reduced referral-to-admission time significantly. You can also review referral management systems that align with your workflow and volume needs.
Frequently asked questions
What is healthcare interoperability and why does it matter for skilled nursing admissions?
Healthcare interoperability is the secure, automated exchange of patient data between hospitals and SNFs or rehab centers, enabling your team to receive complete clinical and insurance information at the point of referral. Interoperability streamlines intake by replacing manual data collection with structured, real-time data flow that speeds up admissions decisions.
How much efficiency gain can SNFs expect with interoperability solutions?
Studies show that real-time interoperability improves efficiency by 15% and can reduce readmission rates by 21 to 29%, with large post-acute care networks reporting up to $8 million in annual savings.
Are there limitations to interoperability’s impact on patient outcomes?
Yes. Some research found no significant reductions in SNF readmissions from health information exchange participation, indicating that outcomes depend heavily on how well the technology is integrated into daily admissions workflows.
What are the highest-ROI workflows for admissions teams using interoperability?
ADT notifications and medication reconciliation are the highest-impact use cases for admissions teams, delivering measurable time savings and cost reductions when prioritized early in implementation.
How can admissions coordinators avoid common interoperability pitfalls?
Focus on workflow-driven implementation and staff engagement rather than treating interoperability as a compliance exercise, since technology access alone does not produce better admissions outcomes without active, consistent use by your team.