
TL;DR:
- Incomplete or inconsistent clinical documentation leads to significant revenue loss and regulatory risks for skilled nursing facilities. Implementing comprehensive knowledge, proper templates, structured formats, ongoing audits, and fostering a culture of accuracy can greatly enhance compliance and reduce denials. Utilizing AI-powered tools like Smart Admissions streamlines intake and documentation workflows, supporting proactive, sustainable adherence to regulatory standards.
Incomplete or inconsistent clinical documentation is one of the most expensive problems your skilled nursing facility faces. Insufficient documentation caused 60.2% of Medicare SNF reimbursement denials in 2021, and recent CERT data shows a 17.2% improper payment rate for SNF services, totaling approximately $5.9 billion, with 79.1% of those errors tied directly to documentation gaps. These are not abstract statistics. They represent revenue your facility has already earned but cannot collect, and regulatory exposure that accumulates with every incomplete record. This article gives your admissions and clinical teams a structured, actionable path to close those gaps and protect your facility’s financial and compliance standing.
Table of Contents
- Understand documentation requirements in skilled nursing facilities
- Core principles of accurate and compliant clinical documentation
- Leverage structured formats, templates, and EHR tools for efficiency
- Audit, verify, and avoid common documentation pitfalls
- The uncomfortable truth about documentation culture: Consistency beats heroics
- Streamline your clinical documentation workflow: Smart solutions for SNFs
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Know all required records | Understand every mandatory documentation element to ensure full compliance. |
| Standardize documentation | Structured templates and EHR tools save time and reduce errors across your facility. |
| Audit routinely | Regular verification and claim scrubbing prevent costly denials and compliance issues. |
| Prioritize consistency | A consistent, prevention-focused documentation culture outperforms periodic ‘catch-up’ efforts. |
| Leverage automation | Automation solutions can streamline workflow, helping teams maintain best practices effortlessly. |
Understand documentation requirements in skilled nursing facilities
The financial risk is real. Before your team can reduce denials, everyone needs a shared understanding of exactly what documentation regulators and payers require at the point of admission and throughout the care episode.
The SNF documentation management guide outlines the full scope of record-keeping obligations for post-acute providers. At the federal level, CMS and Medicare set minimum standards, but state agencies and accreditation bodies like The Joint Commission layer on additional requirements. Understanding all three levels is essential.
According to the CMS Documentation Matters Toolkit, records must meet professional standards and be available and accurate during surveys, with most state and federal regulations requiring retention of five years or more. Failing an audit because a record is missing or incomplete is entirely preventable when the right systems are in place.
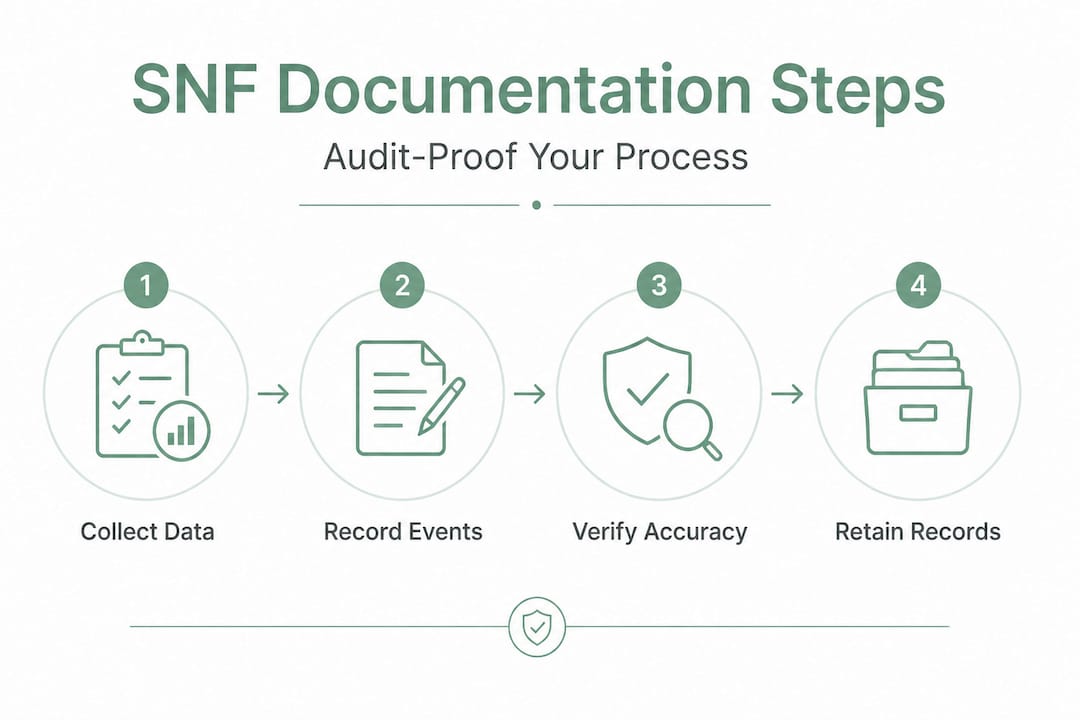
Here is what your facility must maintain for every admission:
- Resident identification documents (name, date of birth, Medicare/Medicaid number)
- MDS/RAI assessments (Minimum Data Set and Resident Assessment Instrument)
- Individualized care plans developed within the required timeframe
- Physician orders and certifications, including initial certification and recertifications
- Progress notes from nursing, therapy, and other disciplines
- Rehabilitation therapy notes documenting functional status and skilled need
- Medication administration records (MAR) and pharmacy review documentation
- Discharge summaries and transfer documentation
The FCSO SNF documentation checklist confirms that required SNF documentation includes all of the above categories, and missing even one element from a claim can trigger a denial or audit finding. Your admissions staff should treat this list as a minimum standard, not a ceiling.
Key compliance reminder: Regulatory surveyors and Medicare auditors look for records that tell a coherent clinical story. Gaps in timing, missing signatures, and contradictions between disciplines are red flags that invite deeper scrutiny.
| Documentation category | Primary driver | Retention minimum |
|---|---|---|
| MDS/RAI assessments | CMS/Medicare | 5 years |
| Physician certifications | Medicare Part A | 5 years |
| Progress notes (nursing) | State licensing + CMS | 5 to 7 years |
| Rehabilitation therapy notes | Medicare + accreditation | 5 years |
| Medication administration records | State pharmacy law | 2 to 7 years (varies) |
| Discharge summaries | CMS + state | 5 years |
Core principles of accurate and compliant clinical documentation
Once you know what’s required, it’s essential to document it the right way. Knowing the required documents is only half the equation. How your team writes those records determines whether a claim survives a review.
Accurate, timely, and objective documentation using specific language without vague terms is the standard CMS and Medicare auditors apply. Every note must be able to stand alone and justify the level of care billed.
The five core principles your team should internalize are:
- Accuracy: Every entry reflects the actual clinical status of the resident, not approximations or assumptions.
- Timeliness: Notes are entered as close to the point of care as possible, ideally in real time, and never backdated.
- Completeness: All required fields, signatures, and supporting details are present before a record is considered closed.
- Legibility: Whether handwritten or electronic, the record must be readable and unambiguous.
- Objectivity: Clinical observations are documented as facts, not interpretations. “Resident refused morning medication stating headache” is objective. “Resident seemed upset” is not.
Language specificity is where many facilities struggle. Vague documentation creates risk. Compare the following examples directly:
| Documentation entry | Type | Why it matters |
|---|---|---|
| “Resident ambulated with assistance” | Problematic | No distance, device, or assistance level specified |
| “Resident ambulated 25 feet with front-wheeled walker and contact-guard assist of one” | Correct | Specific, measurable, demonstrates skilled need |
| “Wound appears to be healing” | Problematic | No measurement, tissue description, or drainage details |
| “Wound measures 2.1 cm x 1.4 cm, 0.3 cm depth; no drainage, granulation tissue visible” | Correct | Objective and complete, supports continued skilled care |
| “Patient doing better today” | Problematic | Subjective and provides no clinical basis for skilled level of care |
| “Patient reports pain 3/10 at rest, 5/10 with movement; responding to current pain management regimen” | Correct | Specific, functional, and clinically relevant |
Pro Tip: After every shift change, have clinical leads do a quick cross-check between progress notes and flow sheets for the same resident. Inconsistencies between these two records are among the most cited audit findings and are entirely preventable with a two-minute verification step.
Leverage structured formats, templates, and EHR tools for efficiency
With core principles established, it is time to work smarter. Structured tools and technology improve documentation quality at scale without adding burden to already stretched clinical staff.
Standardized formats like SOAP notes, structured templates, and EHR tools improve efficiency, reduce errors, and support completeness. SOAP stands for Subjective, Objective, Assessment, and Plan. This format guides clinicians through a logical sequence that ensures nothing is left out and the clinical reasoning is visible to auditors and payers.
A PMC study on note completeness found that structured templates and targeted training significantly improved note completeness across key documentation categories including medication history and clinical background. The same research points to AI and EHR tools capable of reducing charting time by up to 90%, which is meaningful for facilities where nursing staff spend hours per shift on documentation alone.
Here is a step-by-step approach to implementing structured documentation in your facility:
- Audit your current templates. Review existing note templates in your EHR against the required documentation checklist. Identify gaps where required fields are missing or optional rather than mandatory.
- Build mandatory fields into your EHR. Work with your EHR vendor to make critical fields required before a note can be signed. This prevents incomplete records from entering the system.
- Create discipline-specific templates. Nursing, therapy, and social work have different documentation needs. Tailor templates to each role while maintaining interdisciplinary consistency.
- Enable real-time documentation prompts. Many EHR systems support alert rules that prompt clinicians to complete missing items before closing a visit. Activate these prompts for high-risk documentation categories like physician orders and therapy assessments.
- Integrate with your existing workflow. Automated skilled nursing documentation solutions that connect to your current EHR reduce duplicate data entry and support faster, more accurate intake processing.
Facilities that invest in intake documentation efficiency at the point of admission set the tone for the entire care episode. When intake records are complete and accurate from day one, downstream documentation is far more likely to follow suit.
Pro Tip: Train staff not just on how to use each EHR field, but on why it matters for reimbursement and compliance. Staff who understand that an incomplete therapy note can cost the facility thousands in denied claims are more motivated to document thoroughly than those who see it as a checkbox exercise.
Efficiency note: Real-time documentation entered at the bedside or within one hour of care delivery is significantly less likely to contain errors than documentation completed at the end of a shift from memory.
Audit, verify, and avoid common documentation pitfalls
Even with the best systems in place, vigilance is required. Documentation quality degrades over time without active monitoring. Your team needs routine processes to catch problems before they become denials.
Physician certification and recertification must demonstrate medical necessity for daily skilled care, be completed within 30 days, and be supported by consistent interdisciplinary documentation. If the physician’s certification says one thing and the nursing progress notes say another, auditors will question the validity of the entire record.
The five most common documentation pitfalls that directly drive denials are:
- Missing or late physician certifications. Certifications not completed within the required window create automatic compliance exposure.
- Copy-paste and cloned notes. Duplicating prior notes without updating content is a major audit red flag. Medicare guidance specifically flags clone documentation as a compliance risk.
- Flow sheet and narrative inconsistencies. When a flow sheet shows a resident declined therapy but the therapy note shows full participation, surveyors notice.
- Post-entry alterations. Editing a record after it has been signed and dated, without a clearly documented addendum, creates legal and compliance risk.
- Interdisciplinary contradictions. When nursing, therapy, and social work notes conflict on the same resident’s status, the overall record loses credibility.
For proactive prevention, implement these audit steps on a regular cycle:
- Weekly claim scrubbing. Review claims for missing signatures, incomplete assessments, and unsupported level-of-care billing before submission.
- Monthly targeted audits. Focus on high-risk documentation categories: therapy notes, physician certifications, and MDS accuracy. Rotate focus areas to cover all categories over a quarter.
- Denial trend analysis. Track denial reasons by category and payer. Patterns in denial data reveal systemic documentation gaps that training or system changes can address.
- Appeal readiness review. For every denial, verify that the record contains sufficient documentation to support an appeal. Facilities with complete records appeal successfully at a much higher rate.
Proactive claim scrubbing and targeted audits on high-risk areas, combined with ongoing denial trend analysis, are the most effective strategies for reducing SNF denials over time.
Connecting your clinical assessment automation workflow to audit functions gives your team real-time visibility into documentation completeness before claims are submitted. And for medication-related documentation specifically, following established medication management best practices ensures your MAR records meet both clinical and compliance standards.
The uncomfortable truth about documentation culture: Consistency beats heroics
Here is what most documentation training misses. The facilities with the cleanest records and the lowest denial rates are not the ones with the most talented staff or the most aggressive catch-up days. They are the ones that have made accurate documentation a non-negotiable daily habit, embedded into every shift, every role, and every system.
The reality is that most documentation failures are process problems, not people problems. When a nurse submits an incomplete note, it is usually because the template did not prompt for the missing field, or the shift ended before the record was finished, or no one ever explained why that specific detail mattered. Blaming staff effort misses the root cause entirely.
Facilities that rely on “documentation sprints” before audits or quarterly clean-up sessions are managing the symptom, not the condition. Those bursts of activity produce temporary improvements that erode within weeks because the underlying daily habits have not changed. Small, consistent documentation wins every day outperform sporadic intensive efforts every time.
Building a culture where every team member genuinely owns documentation quality requires three things. First, leadership must model the behavior. When administrators and DONs treat documentation standards as a genuine priority rather than a compliance checkbox, staff follow. Second, feedback must be immediate and specific. Telling a clinician three weeks after the fact that their notes were incomplete does not change behavior. Real-time or same-shift feedback does. Third, the systems must support the standards. If your EHR makes it easier to skip a field than to complete it, documentation quality will suffer regardless of staff intentions.
Automated documentation advantages extend beyond time savings. When your systems enforce completion requirements at the point of entry, you remove the dependence on individual vigilance and create structural compliance. That is far more sustainable than relying on heroics.
Streamline your clinical documentation workflow: Smart solutions for SNFs
A prevention-focused culture thrives with the right tools behind it. If your facility is ready to move from reactive documentation management to proactive, system-supported compliance, Smart Admissions is built for exactly that.
Smart Admissions is an AI-powered admissions and referral management platform designed specifically for skilled nursing facilities and rehabilitation centers. It integrates with your existing EHR to automate intake documentation, verify patient eligibility in real time, and reduce the administrative burden that leads to documentation errors. When your team has the right information at the right time, documentation accuracy improves naturally.
If you are ready to automate your admissions process and see faster bed occupancy with fewer denials, explore how referral management systems can connect your intake workflow end to end. Visit Smart Admissions to see how facilities like yours are achieving measurable efficiency gains without overhauling their existing systems.
Frequently asked questions
What documentation is required for SNF Medicare reimbursement?
Facilities must maintain resident ID, assessments, care plans, progress notes, physician certifications, orders, rehab notes, medication records, and discharge summaries to meet Medicare reimbursement requirements.
How can EHR and templates improve SNF documentation?
Standardized EHR templates ensure completeness, reduce documentation errors, and according to a PMC study on charting time, AI and EHR tools can cut charting time by up to 90%.
What are common causes of SNF documentation denials?
Insufficient clinical documentation is the leading cause, accounting for 60.2% of Medicare SNF denials in 2021 and 79.1% of improper payment errors in recent CERT data.
How often must physician certifications be updated for SNF care?
Physician certification or recertification must be obtained within 30 days and must be supported by consistent interdisciplinary documentation to satisfy Medicare requirements.
What audit strategies help prevent reimbursement denials?
Regular claim scrubbing, targeted audits, and systematic denial trend analysis across high-risk documentation areas are the most effective strategies for reducing denials and strengthening your appeals process.