
TL;DR:
- The referral-to-admission conversion rate at skilled nursing facilities has declined significantly, impacting revenue and operational efficiency. Incorporating faster workflows, improved data interoperability, and strict regulatory compliance are essential for success in 2026. Facilities that optimize referral handling, documentation, and regulatory adherence will gain competitive advantages amid rising occupancy and shifting payment models.
The referral-to-admission conversion rate at skilled nursing facilities (SNFs) dropped to a historic low of 23.6% in 2022, and even at its best, never exceeded 37%. For admissions directors, that number represents far more than a statistic. It reflects lost revenue, unfilled beds, and operational strain that ripples across your entire facility. In 2026, the dynamics are shifting, but capturing those gains requires more than just waiting for referrals to arrive. Your team needs sharper tools, faster workflows, and a firm grasp on the regulatory and financial forces reshaping the post-acute care landscape.
Table of Contents
- Admissions trends: Key data shaping 2026
- Why referral conversion economics matter more than ever
- Regulatory updates and financial pressures for 2026
- Interoperability and workflow: The final conversion obstacles
- Special case: IRF admission compliance and documentation readiness
- Our perspective: The hidden differentiators in 2026 admissions success
- Transform your admissions process for 2026 success
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Referral conversion rising | 2026 brings higher referral-to-admission rates for SNFs, underscoring the need for conversion-focused intake. |
| Occupancy trends up | More facilities operate at high census, so responsiveness and intake quality are vital differentiators. |
| Regulatory and financial shifts | CMS payment updates and VBP reductions increase the importance of compliance and payer strategy. |
| Interoperability gaps persist | Workflow and data exchange obstacles can still limit admissions efficiency if not proactively addressed. |
| Documentation powers compliance | IRF and all admissions must prioritize timely, thorough records to avoid denials and optimize revenue. |
Admissions trends: Key data shaping 2026
Building on that preview of major shifts, the numbers defining healthcare admissions in 2026 tell a compelling story of recovery and rising competitive pressure.
Referral acceptance rates have rebounded meaningfully. The acceptance rate reached ~32% in 2024, up from the 2022 low, though still far below what most facilities need to operate at peak efficiency. This means roughly two out of every three referrals your team receives still do not convert to an admission. Every missed conversion represents a missed revenue opportunity and an unfilled bed.
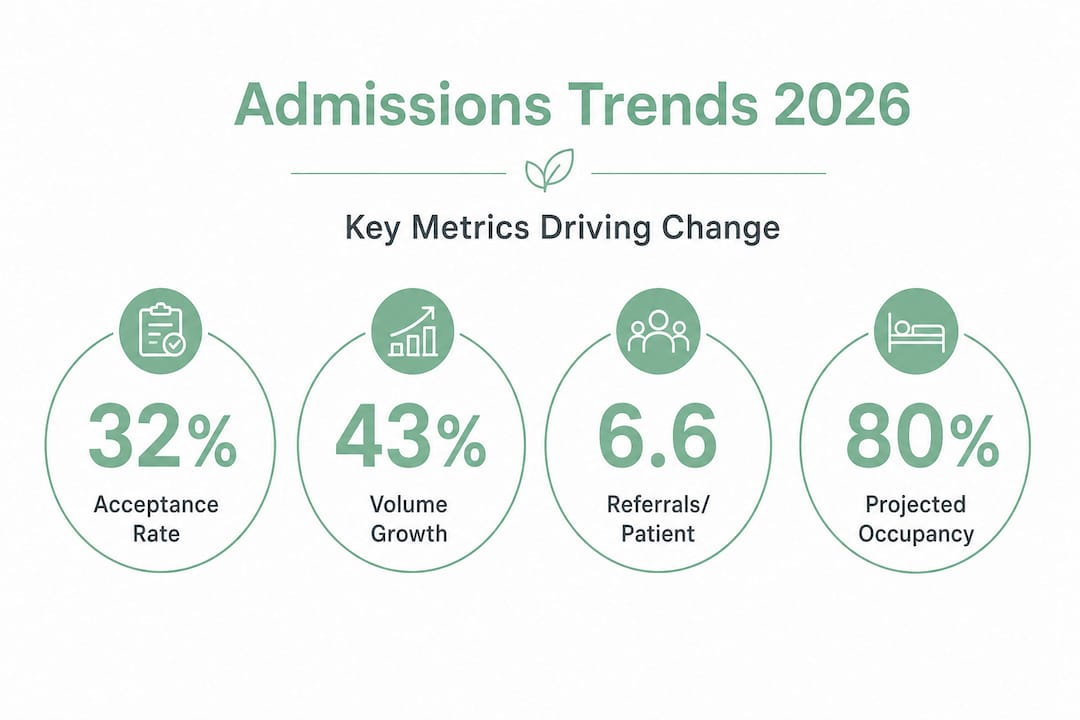
Admission volumes are climbing at the same time. Total patients accepted and admitted have grown nearly 43% since 2019, driven by an aging population, shorter hospital stays, and stronger physician and case manager relationships with SNF networks. SNF occupancy is forecast to reach 80 to 81% nationally in 2026, with a growing number of facilities operating at 85% or higher census. Fewer facilities will fall below the 70% mark, which has historically represented a financial warning zone.
| Metric | 2022 | 2024 | 2026 Forecast |
|---|---|---|---|
| Referral acceptance rate | 23.6% | ~32% | Trending upward |
| Admitted patients growth vs. 2019 | Baseline recovery | +43% | Continued growth |
| National SNF occupancy | ~75% | ~78% | 80–81% |
| Facilities at 85%+ occupancy | Minority | Growing | More widespread |
What do these numbers mean operationally? Two things stand out. First, the facilities winning in this environment are not simply receiving more referrals. They are converting a higher percentage of the referrals they already get. Second, occupancy pressure means the margin for slow response times is shrinking. When a hospital discharge coordinator sends a referral packet, the facilities that respond within minutes, not hours, are the ones filling beds.
Improving your referral conversion efficiency is no longer optional for high-performing SNFs. It is a core operational competency. Avoiding common admissions process pitfalls that slow your team’s response time directly affects your census numbers and your bottom line.
“The facilities best positioned for 2026 are those that treat referral review speed and intake quality as clinical priorities, not administrative afterthoughts.”
Why referral conversion economics matter more than ever
With the data established, it is important to unpack what these shifts in referral and admission rates mean for day-to-day economics and facility competitiveness.
Consider the volume involved. Providers submitted 6.6 referrals per patient on average in 2024. That means for every patient who ultimately gets admitted to your facility, nearly seven referral reviews were conducted somewhere in the process. Your team is competing for each patient against multiple other facilities, often simultaneously. Speed, accuracy, and responsiveness determine who wins that admission.
The economics of conversion are straightforward but often underestimated. If your facility receives 100 referrals per month and converts at 30%, you are admitting 30 patients. If you improve your conversion rate to 38% with better workflows and faster response times, that is eight additional admissions per month. At an average Medicare daily rate, those additional admissions can represent hundreds of thousands of dollars in annualized revenue.
To build a conversion-focused operation, your team should measure and actively manage each stage of the referral funnel:
- Referrals received – Total volume of incoming referral packets from hospitals, discharge planners, and physician offices.
- Referrals reviewed – Time from receipt to clinical review completion, including documentation assessment.
- Referrals accepted – The percentage your team accepts after clinical and payer eligibility review.
- Patients admitted – The conversion from acceptance to actual admission, tracking any drop-off due to patient or family decisions.
- Denial root cause tracking – Categorizing why referrals are declined, whether due to clinical complexity, payer mismatch, or documentation gaps.
| Funnel stage | Common failure point | Improvement lever |
|---|---|---|
| Referral received to reviewed | Slow manual triage | Automated routing and alerts |
| Reviewed to accepted | Incomplete clinical data | EMR integration for real-time access |
| Accepted to admitted | Coordination delays | Digital scheduling and communication tools |
| Post-admission denials | Documentation errors | Standardized intake checklists |
Pro Tip: Conduct a monthly audit of your admissions funnel. Break down where referrals are being lost, whether at the review stage, the acceptance stage, or post-acceptance. You cannot fix what you are not measuring. Many facilities discover that their biggest drop-off is not at the clinical review stage but in the coordination gap between acceptance and actual admission.
Adopting better referral strategies for better bed fill and aligning your team around structured referral conversion strategies are both proven ways to tighten up each stage of the funnel.
Regulatory updates and financial pressures for 2026
Understanding the financial landscape is crucial to seeing how regulatory changes force new operational priorities in admissions.
The Centers for Medicare and Medicaid Services (CMS) finalized its Fiscal Year 2026 Skilled Nursing Facility Prospective Payment System (SNF PPS) rule with significant implications for your facility’s financial planning. The FY 2026 SNF PPS rates were updated by 3.2%, translating to an overall payment increase of approximately $1.16 billion compared to FY 2025. However, the headline number does not tell the full story.
The SNF Value-Based Purchasing (VBP) program, which ties a portion of Medicare payments to performance on rehospitalization metrics, will apply reductions totaling $208.36 million across the sector. That means facilities that are not actively managing their readmission rates and clinical outcomes will see a direct hit to their Medicare revenue. The VBP multiplier creates a scenario where even a 3.2% rate increase can be partially or fully offset by performance-based reductions.
For your admissions team, this regulatory environment creates several strategic imperatives:
- Payer mix optimization. Evaluate your current ratio of Medicare, Medicaid, and private pay admissions. Higher-acuity Medicare patients typically drive better per-diem rates, but they also carry higher documentation burdens and readmission risks.
- Denial prevention as a financial priority. Every denied claim represents revenue already earned but not collected. Upstream improvements to intake documentation directly reduce downstream denial rates.
- Clinical complexity thresholds. With VBP pressures on readmissions, your clinical admissions criteria should align with what your facility can safely manage, not just what increases census.
- Referral source relationship management. Hospitals tracking their post-acute partner performance will increasingly direct referrals to facilities with stronger outcomes. Your admissions quality affects your referral pipeline.
“Regulatory compliance and admissions quality are not separate concerns. Facilities that treat documentation and payer strategy as admissions functions will outperform those that treat them as billing-only problems.”
Pro Tip: Pull a denial report by payer type at least quarterly. Identify whether denials cluster around specific payer requirements, clinical documentation gaps, or eligibility verification errors. Then adjust your intake workflow to address those patterns before they become patterns of lost revenue. Reviewing your intake optimization strategies can give your team a practical framework to reduce preventable denials systematically.
Interoperability and workflow: The final conversion obstacles
Even with strategic planning, workflow execution can break down at the point of data exchange, making conversion obstacles a critical focus for 2026.
Here is a number that should concern every admissions director: only 55% of hospitals can reliably find, send, receive, and integrate patient information electronically with nursing homes. That means in nearly half of all hospital-to-SNF transitions, your team is working with incomplete, delayed, or manually transmitted information. Fax machines, phone tag, and PDF attachments are still the standard in too many referral workflows.
This interoperability gap has direct consequences for your conversion rate. When your admissions coordinator cannot access a complete clinical picture quickly, review times slow down. When documentation arrives in pieces across multiple channels, errors accumulate. When eligibility verification requires manual portal checks, response time increases. Each delay gives competing facilities an opportunity to accept the patient first.
The practical impact of poor interoperability includes:
- Extended referral review cycles because clinical data arrives incomplete or requires manual assembly.
- Duplicate data entry across your EMR, admissions software, and payer portals, which increases error risk and staff workload.
- Delayed eligibility verification, which creates uncertainty about whether the admission will be covered before bed assignment.
- Communication gaps between the hospital discharge team and your admissions staff, leading to last-minute surprises at the point of transfer.
“Data fragmentation is not a technology problem. It is a revenue problem. Every hour of delay in referral review is an hour that competing facilities use to fill their beds.”
Solutions your facility should evaluate for 2026 include electronic medical record (EMR) integration with referral management platforms, digital referral intake portals that standardize incoming documentation, real-time insurance eligibility verification tools, and workflow automation that routes referral packets to the right clinical reviewer without manual triage. Implementing streamlining administrative tasks across your intake workflow eliminates the manual bottlenecks that slow conversion and drain your admissions staff.
Special case: IRF admission compliance and documentation readiness
For facilities also managing inpatient rehabilitation facility (IRF) beds, admissions success hinges on stricter compliance and documentation controls, requiring a parallel but distinct workflow from your SNF admissions process.
Medicare’s IRF coverage requirements are detailed and non-negotiable. The preadmission screening must occur within 48 hours immediately preceding the IRF admission and must be conducted by a licensed clinician. This screening serves as the primary documentation of medical necessity and directly determines whether Medicare will cover the admission. If the timing or content of the screening is inadequate, your facility faces denial risk regardless of the patient’s clinical appropriateness.
IRF compliance requires a structured, repeatable process at every admission. Your team should follow these steps for every Medicare IRF case:
- Confirm IRF eligibility criteria before the screening appointment. Verify that the patient meets the requirement for intensive therapy, defined as at least three hours of therapy per day, five days per week, under a physician’s supervision.
- Schedule the preadmission screening within the 48-hour window and assign a licensed clinician who understands IRF documentation requirements.
- Complete the Inpatient Rehabilitation Facility Patient Assessment Instrument (IRF-PAI) accurately and in full, as errors here directly affect case mix group assignment and payment.
- Document the individualized overall plan of care with specific functional goals, anticipated length of stay, and discharge planning details.
- Conduct the post-admission physician evaluation within 24 hours of admission, and document it as a separate clinical note from the preadmission screening.
Pro Tip: Build a templated documentation checklist specific to IRF admissions and attach it to every IRF referral as it enters your intake system. The checklist should include the 48-hour screening window, IRF-PAI completion, therapy intensity documentation, and physician evaluation timing. Reviewing your approach to optimizing IRF admissions through structured intake tools significantly reduces the risk of costly post-admission denials.
Our perspective: The hidden differentiators in 2026 admissions success
Having covered the what and how of 2026 admissions trends, it is worth sharing a deeper perspective on what actually separates leaders from laggards in this environment.
Most conversations about SNF admissions performance focus on referral volume. Facilities ask how to get more referrals from more hospitals. That is the wrong question. The facilities outperforming their peers in 2026 are not necessarily receiving more referrals. They are converting a higher percentage of the referrals they already receive, and they are doing it faster and with fewer downstream errors.
The real differentiator is end-to-end workflow speed paired with intake quality. A facility that reviews a referral in 20 minutes with complete clinical documentation has a significant advantage over one that takes two hours with incomplete data. That speed gap compounds over months into a measurable census advantage and a stronger referral relationship with hospital discharge teams who notice which facilities respond reliably.
There is also an underappreciated value in audit-driven process improvement. Facilities that regularly review their denial patterns, funnel drop-off rates, and payer-specific documentation requirements develop a compounding operational advantage. Each improvement cycle tightens the intake workflow incrementally. Over a year, those incremental gains translate into material revenue improvement and lower administrative costs per admission.
Perhaps most importantly, digital readiness remains the single largest lever for competitive advantage in 2026. Facilities that have integrated their EMR with digital referral management platforms, automated eligibility verification, and structured documentation workflows are operating at a fundamentally different efficiency level than those relying on manual processes. The technology gap between digitally mature facilities and those still relying on fax-based workflows is widening, not narrowing.
If you want to understand how far this can go, reviewing what AI in referral management makes possible in terms of speed and accuracy is a useful starting point. The facilities investing in these capabilities now will hold a structural advantage as occupancy pressures intensify across the sector.
Transform your admissions process for 2026 success
The trends, regulations, and workflow challenges outlined in this guide all point to one conclusion: your admissions process is one of the highest-leverage operational areas in your facility, and 2026 demands that it perform at a higher level than ever before.

Smart Admissions is built specifically for skilled nursing and rehabilitation facilities navigating exactly these challenges. The platform’s AI-powered referral management tools connect your intake automation solutions with real-time eligibility verification, clinical documentation management, and EMR integration. Your team gets faster referral reviews, fewer manual steps, and better data at every stage of the funnel. Explore how workflow optimization tools can reduce your review cycle times, and see how easy it is to integrate EMR with referrals to eliminate data fragmentation from your intake process. Your 2026 performance starts with your admissions workflow.
Frequently asked questions
What is the average referral to admission conversion rate for SNFs in 2026?
The average acceptance rate is approximately 32% as of 2024, and it continues trending upward. Facilities with faster review times and stronger documentation quality consistently perform above this average.
How is SNF occupancy changing in 2026?
National SNF occupancy is projected to reach 80 to 81% in 2026, with more facilities operating at 85% or higher census and fewer falling below the 70% threshold that signals financial risk.
What new financial pressures affect admissions in 2026?
CMS updated SNF PPS rates by 3.2% for FY 2026, but VBP reductions totaling $208.36 million mean facilities with higher readmission rates will see their payment increases reduced or eliminated entirely.
What’s the biggest workflow challenge for facility admissions?
Limited interoperability is a primary barrier, given that only 55% of hospitals can reliably exchange patient data electronically with SNFs, which slows referral review and increases administrative errors.
How can IRFs improve admissions compliance for Medicare?
IRFs must ensure that preadmission screening occurs within 48 hours before admission and that all documentation is completed accurately to establish medical necessity and avoid costly claim denials.