
TL;DR:
- Skilled nursing admission processes are complex, involving clinical, regulatory, and financial assessments to ensure compliance and efficiency.
- Most bottlenecks stem from incomplete evaluations, misaligned payer requirements, and clinical misconceptions, which can lead to denials and delays.
Skilled nursing facility admissions are far more involved than matching an open bed to an available patient. Your team must evaluate clinical needs, verify insurance eligibility, satisfy federal and state regulatory requirements, and manage payer mix, all within tight hospital discharge timelines. Each decision carries real financial and compliance consequences. This guide walks through every critical phase of the admissions process, from pre-admission screening to care planning, so your facility can make faster, more confident decisions while reducing the risk of denials and regulatory setbacks.
Table of Contents
- The admissions decision-making framework: From screening to care planning
- Navigating regulatory and eligibility requirements: CMS, PASRR, and Medicaid
- Financial considerations: Payer mix, occupancy strategies, and prioritization
- Clinical appropriateness and workflow pitfalls: Avoiding referral errors
- A fresh perspective: What most administrators overlook about admissions decision-making
- Next steps: Streamline your admissions with expert solutions
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Multiphase admissions workflow | The admissions process includes screening, assessment, financial checks, contracts, and care planning. |
| Regulatory and eligibility checks | CMS, PASRR, and Medicaid rules determine who qualifies and can delay or deny admissions if unmet. |
| Financial and occupancy strategies | Payer mix and real-time occupancy drive prioritization and successful admissions outcomes. |
| Clinical appropriateness matters | Ensuring candidates meet medical necessity prevents referral errors and optimizes facility resources. |
| Tech tools improve efficiency | Integrated platforms and automated workflows help admissions teams reduce delays and compliance risks. |
The admissions decision-making framework: From screening to care planning
After you recognize the full complexity of admissions, the next step is mapping out each phase so your team knows exactly what to evaluate and when. Admissions process optimization starts with understanding how each stage connects to the next.
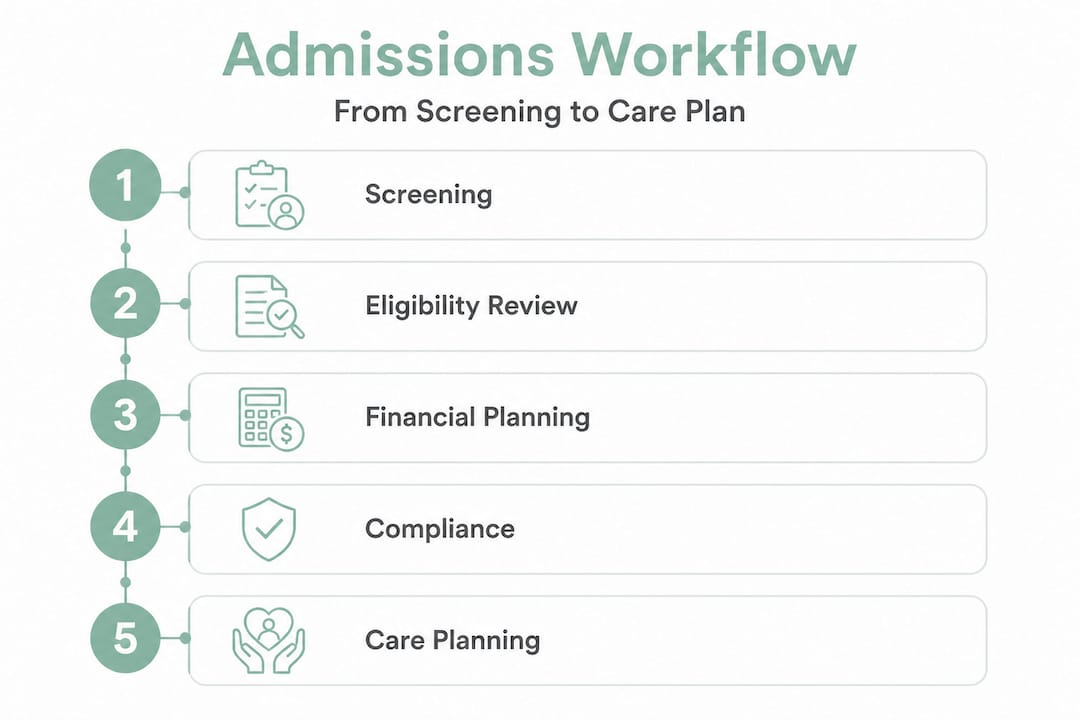
The multi-phase admissions process covers pre-admission screening, clinical assessment using tools like the Minimum Data Set (MDS), financial and payer verification, contract execution, and initial care planning. Missing or rushing any one of these phases creates downstream problems that affect care quality, compliance, and revenue.
Here is how each phase breaks down in practice:
- Pre-admission screening: Your team reviews referral documents, hospital records, and preliminary diagnoses to determine whether the patient’s care needs match your facility’s capabilities and licensure.
- Clinical assessment using MDS: The Minimum Data Set is a standardized federal tool used to assess a resident’s functional, cognitive, and medical status. Completing it accurately drives reimbursement rates under the Patient-Driven Payment Model (PDPM).
- Financial and payer verification: Staff confirm insurance coverage, prior authorization requirements, benefit days remaining, and estimated payment rates before a bed is committed.
- Contract execution: Admission agreements, financial responsibility disclosures, and rights notifications must be reviewed and signed in accordance with CMS regulations.
- Initial care planning: A preliminary interdisciplinary care plan is established within 48 hours of admission, aligning clinical goals with the resident’s assessed needs.
The table below summarizes the key tools and processes used at each phase:
| Phase | Primary tools | Key compliance requirement |
|---|---|---|
| Pre-admission screening | Referral documents, EHR review | Licensure and scope of care match |
| Clinical assessment | MDS 3.0, PDPM calculation | Federal assessment schedules |
| Financial verification | Insurance portals, eligibility tools | Prior authorization, benefit confirmation |
| Contract execution | Admission agreements, rights forms | CMS conditions of participation |
| Initial care planning | Interdisciplinary care plan template | 48-hour care plan requirement |
Strong decision-making in admissions depends on each team member understanding their role in this sequence. When phases are completed in parallel rather than sequentially, your facility reduces delays without cutting corners. Automated workflow automation insights show that facilities using structured intake checklists significantly reduce documentation errors and speed up time to bed assignment.
Navigating regulatory and eligibility requirements: CMS, PASRR, and Medicaid
With the process map in mind, let’s focus on the regulatory hurdles that most frequently create bottlenecks in admissions eligibility decisions.
Medicare Part A SNF coverage requirements
Medicare Part A SNF coverage requires four conditions to be met: a prior 3-day inpatient hospital stay, transfer to the SNF within 30 days of hospital discharge, a daily skilled nursing or therapy need that is directly related to the hospitalization, and physician certification of that need. If any one of these criteria is not met, Medicare will not cover the stay, and your facility absorbs the financial risk if the patient cannot self-pay.

Common mistakes at this stage include counting observation stays toward the 3-day inpatient requirement, which CMS does not allow. Patients and families often do not realize their hospital status was “under observation” rather than formally admitted. Training your admissions staff to verify inpatient status directly through the hospital’s billing department prevents this costly error. You can also review Medicare nursing home coverage resources to clarify these rules for families during the intake conversation.
Medicaid functional eligibility and level of care
Medicaid long-term care eligibility generally requires functional impairment in three or more Activities of Daily Living (ADLs), as determined through a state-specific Level of Care (LOC) evaluation, when services cannot reasonably be provided in a community setting. ADLs include bathing, dressing, toileting, transferring, continence, and eating. Each state defines its LOC criteria slightly differently, so your admissions team must stay current with your state’s specific thresholds.
For facilities accepting Medicaid residents, Medicaid eligibility guidance should be part of your standardized intake review to avoid accepting residents whose eligibility has not yet been confirmed at the state level.
PASRR requirements for Medicaid nursing facility admissions
PASRR screening is mandatory for all Medicaid nursing facility admissions and is designed to screen for serious mental illness (SMI) and intellectual or developmental disabilities (ID/DD). Level I screening identifies cases that may require further evaluation, triggering a Level II assessment conducted by a state-designated entity. The Level II process determines whether the nursing facility is the least restrictive appropriate setting for that individual.
PASRR delays are one of the most common bottlenecks in Medicaid admissions. If your team does not initiate the Level I screening immediately upon receiving a referral, the entire timeline shifts. Facilities that wait for hospital discharge to begin PASRR often face multi-day delays.
Key regulatory requirements to monitor:
- Medicare inpatient stay status must be formally verified, not assumed
- State LOC evaluations must be current and on file before Medicaid billing begins
- PASRR Level I must be initiated at the referral stage, not after admission
- Physician certification of skilled need must be documented and dated prior to admission
Pro Tip: Build a standardized eligibility checklist into your intake workflow that flags PASRR triggers automatically when a referral includes a mental health or developmental disability diagnosis. Automation tools that scan referral documents for these indicators can reduce manual screening time by a significant margin.
Financial considerations: Payer mix, occupancy strategies, and prioritization
Understanding eligibility is necessary, but financial realities often determine which patients move forward. Bed occupancy optimization requires your facility to balance clinical need with payer source, acuity level, and available staffing.
Why payer mix matters
Facilities closely manage payer mix because Medicaid reimbursement rates are substantially lower than Medicare or private pay rates. When a facility’s census is dominated by Medicaid residents, operating margins narrow significantly, making it harder to fund staffing, equipment, and capital improvements. As a result, many facilities prioritize Medicare and private pay admissions when multiple referrals arrive simultaneously, which can create waitlists for Medicaid applicants.
This is not simply a financial preference. It reflects the reality that a facility must remain financially viable to continue serving any residents at all.
National occupancy and payer trends
National SNF occupancy averaged between 79% and 84% from 2023 through 2026. Medicaid covers approximately 63% of resident days, while Medicare accounts for only 8% to 14% of resident days but contributes a disproportionately higher share of facility revenue. SNF admissions per 1,000 fee-for-service beneficiaries dropped to 47 in 2023, representing a 12% decline from 2022, reflecting both demographic shifts and post-pandemic changes in care patterns.
“Medicare covers a small fraction of total resident days in skilled nursing facilities, yet it delivers a revenue share far greater than its volume would suggest. Every Medicare admission that is delayed or denied has an outsized financial impact on your facility’s bottom line.”
Strategic occupancy management
Smart admissions teams use real-time occupancy data to forecast bed availability and match incoming referrals to the highest-value opportunities. Key financial edge cases that require careful management include:
- Skilled vs. custodial care distinction: Medicare covers skilled care only, not custodial support such as help with daily activities. Admitting a patient who only needs custodial care under a Medicare authorization creates a billing error risk and potential recoupment.
- Setting appropriateness: If home health or assisted living can adequately meet the patient’s needs, SNF admission may be denied on appeal.
- Payer mix and capacity limits: Facilities with managed care contracts must also monitor contract-specific authorization requirements, which vary by insurer.
- PASRR-positive screens: A positive PASRR screen can delay admission by days or weeks if not managed proactively.
Pro Tip: Use real-time occupancy dashboards integrated with your EHR to forecast potential gaps in census two to four weeks out. Predictive models that incorporate average length of stay by diagnosis can help your admissions team prioritize referrals that match upcoming availability, rather than reacting to vacancies after the fact.
Clinical appropriateness and workflow pitfalls: Avoiding referral errors
While financial and regulatory factors play a significant role, referral errors in clinical appropriateness can undermine the entire admissions decision. Accepting a patient who does not meet clinical criteria for skilled nursing care leads to denied claims, appeals, staff frustration, and potential compliance citations.
Common clinical referral mistakes
Research on admissions criteria shows that referring provider misconceptions about SNF and inpatient rehabilitation facility (IRF) criteria frequently result in inappropriate referrals. Physicians and case managers at the referring hospital may not fully understand the distinction between skilled need and custodial need, or they may assume that any patient requiring post-acute support qualifies for skilled nursing. A physiatrist or clinical admissions specialist must ultimately determine medical appropriateness beyond what the insurer’s utilization review alone would flag.
“Clinical appropriateness is not just a Medicare billing requirement. It is the foundation of safe and effective post-acute care placement. Admitting a patient to a setting that cannot adequately serve their needs increases readmission risk and compromises outcomes.”
Steps to prevent inappropriate admissions
Follow this structured review process to catch referral errors before bed assignment:
- Initial clinical screening: Review the referral packet for primary diagnosis, functional status, and skilled care needs. Flag any referrals where the documented need appears custodial rather than skilled.
- Physician or nurse practitioner review: Have a licensed clinician evaluate the medical appropriateness of the admission, not just the admissions coordinator.
- Payer coverage cross-check: Confirm that the documented clinical need aligns with the payer’s coverage criteria. Medicare, Medicaid, and managed care organizations all have different standards.
- Setting appropriateness assessment: Determine whether home health, assisted living, or outpatient therapy could meet the patient’s needs. Document your reasoning if SNF is selected over a lower-acuity setting.
- Interdisciplinary team sign-off: Before finalizing the admission, route the referral through a brief interdisciplinary review that includes nursing, therapy, and social work input.
- Documentation audit: Confirm that physician orders, skilled need justification, and payer authorization are all on file before the patient arrives.
This process adds minimal time when supported by structured intake tools, and it significantly reduces post-admission denials and retroactive reviews.
A fresh perspective: What most administrators overlook about admissions decision-making
Here is what industry experience consistently reveals: most admissions problems are not caused by staff incompetence or poor intentions. They are caused by a structural gap between the speed hospitals demand and the thoroughness that compliance and clinical quality require.
Hospitals face intense pressure to discharge patients within 24 to 48 hours of stabilization. That pressure transfers directly to your admissions team in the form of urgent referral calls, incomplete documentation packets, and requests to “just get the patient in.” When teams comply without completing proper eligibility and clinical review, they accept financial and regulatory risk that surfaces weeks later in the form of denied claims and audit findings.
The uncomfortable truth is that many facilities have built their admissions workflows around speed rather than accuracy. That was a reasonable adaptation to competitive referral markets, but it is no longer sustainable. CMS audit activity, managed care utilization reviews, and value-based care incentives all reward accuracy and appropriateness, not just throughput.
What separates high-performing facilities is their investment in optimizing admissions through tools that automate the repetitive verification tasks so that human judgment can focus on the genuinely complex decisions. When your team is not manually calling insurance portals to check benefit days, they have capacity to thoughtfully evaluate clinical appropriateness, identify PASRR triggers, and communicate clearly with referring hospitals.
Integrating AI-assisted tools with your EHR, standardizing your MDS-based clinical review process, and training staff on current Medicare and Medicaid criteria are not optional upgrades. They are the baseline for managing admissions decision-making effectively in 2026 and beyond.
Next steps: Streamline your admissions with expert solutions
The challenges covered in this guide, from regulatory compliance to payer mix management and clinical accuracy, are exactly the problems that modern admissions technology is built to address.

Smart Admissions gives your team a structured admissions workflow guide that connects referral intake, eligibility verification, clinical assessment, and documentation management in one platform. Our AI-powered tools integrate with your existing EHR and insurance portals, enabling real-time verification and reducing manual follow-up time. With admissions automation built into your intake process, your staff spends less time on phone calls and paperwork and more time on decisions that require clinical expertise. Explore referral management examples to see how facilities like yours have improved bed fill rates and reduced denials.
Frequently asked questions
What are the minimum requirements for Medicare SNF admissions?
Medicare SNF admissions require a prior 3-day inpatient hospital stay, transfer within 30 days of discharge, a skilled nursing or therapy need related to the hospitalization, and physician certification. Observation stays do not count toward the 3-day inpatient requirement.
How does PASRR impact Medicaid admissions?
PASRR ensures residents with serious mental illness or intellectual and developmental disabilities are placed in the most appropriate and least restrictive setting, which can trigger state-level Level II evaluations that delay Medicaid admissions if not initiated early in the referral process.
What is the difference between skilled and custodial care?
Skilled care includes medical treatment and therapy services that Medicare will cover, such as wound care, IV therapy, and physical rehabilitation, while custodial care refers to assistance with daily living activities that Medicare does not reimburse.
Why do facilities prioritize certain payers over others?
Facilities prioritize Medicare and private pay admissions because reimbursement rates are significantly higher than Medicaid, which is essential for maintaining operating margins and funding quality care across the entire resident population.
What role does clinical appropriateness play in admissions decisions?
Clinical appropriateness ensures that admitted patients genuinely require skilled nursing services, which protects your facility from denied claims, reduces readmission risk, and ensures that each resident receives care in the setting best suited to their medical needs.